

The anatomical variations of pancreatic duct in the patients with pancreatic diseases


Abstract
There are many anatomic variations of pancreatic duct and congenital anomalies of pancreas, which have been described in the literature. Most of them has no clinical significance and is used to be incidentally discovered in radiological examinations. We have demonstrated in our paper that the most frequent anatomical variations of pancreatic duct in the patients with pancreatic diseases are pancreas divisum as well as ansa pancreatica.
Citation
Jagielski M, Smoczyński M, Adrych K. The anatomical variations of pancreatic duct in the patients with pancreatic diseases. Eur J Transl Clin Med. 2018;1(1):63-66









Many anatomical variations of the pancreatic duct and congenital anomalies of pancreas have been described in the literature [1-5]. Most of them have no clinical significance and are incidentally discovered in radiological examinations [1-2]. Anatomic variants of the main pancreatic duct (MPD) are rarely diagnosed in asymptomatic patients, because most often there is no need to perform pancreatic imaging examinations this particular group of patients.
Endoscopic treatment of pancreatic diseases include procedures that facilitate pancreatic juice outflow [5-7]. Endoscopic retrograde cholangiopancreatography (ERCP) is the gold standard for the evaluation of pancreatic ductal system in the patients suffering from pancreatic diseases, who require endoscopic treatment [6-7]. To assess the MPD in asymptomatic patients who do not need endoscopy, it is recommended to perform secretin-stimulated magnetic resonance cholangiopan reatography (secretin MRCP) [8-10]. Secretin MRCP is considered to be a safe and non-invasive imaging technique, which visualizes the entire pancreatic anatomy, including the ducts.
We conducted retrospective analysis of 2843 endoscopic retrograde pancreatography (ERP) procedures at the Gastrointestinal Endoscopy Unit of our medical center. In the years 2001-2017, a total of 2843 ERP procedures were carried out, resulting in MPD stenting in 688 patients (506 men, 182 women; mean age 44.53 {19–82} years).
Figure 1. Patient with chronic pancreatitis and incomplete pancreas divisum in fluoroscopy image
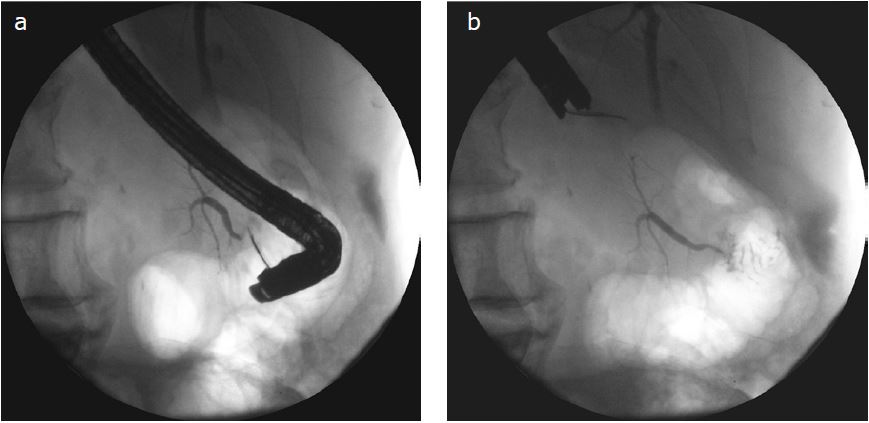
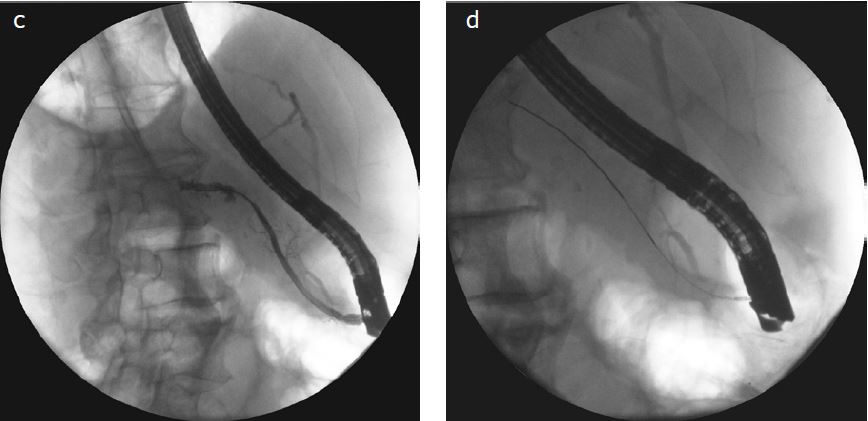
Figure 2a-d. Complete pancreas divisum. Contrast medium applied via major duodenal papilla filled the ventral pancreatic ducts (Fig. 2a,b), while the contrast applied via minor duodenal papilla filled the MPD in the dorsal pancreas (Fig. 2c). A guidewire was introduced into the main pancreatic duct via minor duodenal papilla (Fig. 2d)
Anatomic variations of MPD were diagnosed in 71 of those 688 patients (10.32%) (40 men, 31 women; mean age 42.36 {26-64} years). The most common variant of the MPD was pancreas divisum, which was recognized in 42 (6.1%) patients. Majority of the patients (28, 4.07%) had incomplete pancreas divisum (Fig.1), while the complete pancreas divisum (Fig.2a-d) was discovered in only 14 (2.03%) patients. The second most frequent anatomic variant of the MPD was ansa pancreatica (28 patients, 4.07%) (Fig.3, 4). Doubling of the MPD in the pancreatic body and tail was observed in 1 (0.15%) patient only.
Figure 3. The patient with ansa pancreatica stated during ERCP. An MPD disruption in the pancreatic tail due to acute pancreatitis was also stated
Figure 4. Ansa pancreatica is visible in fluoroscopic image in ERCP
58 (81.69%) of the 71 patients with anatomic variant of pancreatic duct had also chronic pancreatitis and required endoscopic treatment. The suspicion of MPD disruption in course of acute necrotizing pancreatitis was an indication for performance of ERP in the remaining 12 (16.9%) patients.
Pancreas divisum was the most frequent anatomic variation of pancreatic duct in the patients with chronic pancreatitis (40/58 {68.97%} patients). By contrast, ansa pancreatica (Fig.5a-b) was the most common variation of pancreatic duct in patients with MPD disruption in course of acute necrotizing pancreatitis (10/12 {83.33%} patients).
Figure 5a, b. Patient with chronic pancreatitis and ansa pancreatica in fluoroscopy during ERCP (Fig. 5a). A guidewire was introduced into the MPD through a loop of pancreatic duct in head of pancreas (Fig. 5b)
The results of our analysis are similar to those presented in current literature [1-2, 11]. The most common variants of the MPD in our sample were pancreas divisum and ansa pancreatica.
The total number of anatomic variations in general population is low, but in patients suffering from pancreatic diseases this rate is much higher [1-4, 11]. According to the current literature, pancreas divisum is the most common anatomic variant of pancreatic duct in the general population [11]. It is caused by a failure to fuse the ventral and dorsal ducts of the embryonic pancreas during embryonic development [1, 11-13]. The patients with complete pancreas divisum have no junction between the dorsal and ventral pancreatic ducts [1, 11-12]. On the other hand, patients with incomplete pancreas divisum usually have small communicating branch between dorsal and ventral pancreatic ducts [1, 12]. Pancreas divisum is a proven cause of recurrent acute pancreatitis [4, 14-15]. Clinical symptoms related with pancreas divisum are considered to be the only indication for an endoscopic treatment [13, 16].
Ansa pancreatica is defined as the presence of a loop of the MPD as an additional curved communicating duct between the ventral and dorsal ducts in the region of the pancreatic head [3, 5, 17]. It is said that ansa pancreatica predisposes to recurrent acute pancreatitis same as pancreas divisum [3, 17]. However, there are no clear guidelines for endoscopic treatment, due to the fact that ansa pancreatica is a much less common anatomic variant of the MPD than pancreas divisum. In our opinion, ERCP should be performed in every symptomatic patients with the ansa pancreatica variant [5].
Doubling of the MPD was observed in only one of our patients, whereas Hać et al. recognized it in 9.9% of 99 adult autopsy patients [18]. Such markedly different resultsare probably caused by the methodology and the study group [18]. It is noteworthy that the authors took advantage of a much more precise pancreatic duct imaging technique and applied it in group of people without pancreatic diseases [18]. Thus, their results refer to general population, whereas our study group consists specifically of patients with pancreatic disease [18].
The MPD imaging technique similar to the one in our paper was utilized by Bang et al. in a study of 582 patients with pancreaticobiliary diseases, in whom both the MPD and the common bile duct were clearly visible in ERCP [19]. In this study, anatomic variations of pancreatic duct was were found in 51 of 582 patients, while 19 of those 51 patients had pancreas divisum recognized (12 complete and 7 incomplete pancreas divisum) [19]. The authors did not show any significant correlations between the anatomy of pancreatic ducts and occurrence of pancreaticobiliary diseases [19]. Both the methodology and the study group there were very similar to ours [19].
We have retrospectively demonstrated that the most frequent anatomic variations of pancreatic duct in the patients with pancreatic diseases are pancreas divisum (usually incomplete) as well as ansa pancreatica.
References
| 1. |
Türkvatan A, Erden A, Türkoğlu MA, Yener Ö. Congenital variants and anomalies of the pancreas and pancreatic duct: imaging by magnetic resonance cholangiopancreaticography and multidetector computed tomography. Korean J Radiol 2013;14(6):905-913.
|
| 2. |
Mortelé KJ, Rocha TC, Streeter JL, Taylor AJ. Multimodality imaging of pancreatic and biliary congenital anomalies. Radiographics 2006;26(3):715-31.
|
| 3. |
Tamaka T, Ichiba Y, Miura Y, et al. Variations of the pancreatic ducts as a cause of chronic alcoholic pancreatitis; ansapancreatica. Am J Gastroenterol 1992;87(6):806.
|
| 4. |
Bang S, Suh JH, Park BK, et al. The Relationship of Anatomic Variation of Pancreatic Ductal System and Pancreaticobiliary Diseases. Yonsei Med J 2006;47(2):243-248.
|
| 5. |
Jagielski M, Smoczyński M, Drelich-Góreczna B, Adrych K. Transduodenal drainage of symptomatic walled-off pancreatic necrosis in a patient with ansapancreatica anatomic variation. Arch Med Sci 2017;13(1):267-269.
|
| 6. |
Varadarajulu S, Bang JY, Phadnis MA, et al. Endoscopic transmural drainage of peripancreatic fluid collections: outcomes and predictors of treatment success in 211 consecutive patients. J Gastrointest Surg 2011;15(11):2080-2088.
|
| 7. |
Trevino JM, Tamhane A, Varadarajulu S. Successful stenting in ductal disruption favorably impacts treatment outcomes in patients undergoing transmural drainage of peripancreatic fluid collections. J Gastroenterol Hepatol 2010;25(3):526-531.
|
| 8. |
Matos C, Metens T, Devière J, et al. Pancreatic duct: morphologic and functional evaluation with dynamic MR pancreatography after secretin stimulation. Radiology 1997;203(2):435-441.
|
| 9. |
Punwani S, Gillams AR, Lees WR. Non-invasive quantification of pancreatic exocrine function using secretin-stimulated MRCP. Eur Radiol 2003;13(2):273-276.
|
| 10. |
Soto JA, Alvarez O, Múnera F, et al. Traumatic disruption of the pancreatic duct: diagnosis with MR pancreatography. AJR Am J Roentgenol 2001;176(1):175-178.
|
| 11. |
Adibelli ZH, Adatepe M, Imamoglu C, et al. Anatomic variations of the pancreatic duct and their relevance with the Cambridge classification system: MRCP findings of 1158 consecutive patients. Radiol Oncol 2016;50(4):370-377.
|
| 12. |
Lehman GA, Sherman S. Diagnosis and therapy of pancreas divisum. Gastrointest Endosc Clin N Am 1998;8(1):55-77.
|
| 13. |
Neuhaus H. Therapeutic pancreatic endoscopy. Endoscopy 2002;34(01):54-62.
|
| 14. |
Richter JM, Schapiro RH, Mulley AG, Warshaw AL. Association of pancreas divisum and pancreatitis, and its treatment by sphincteroplasty of the accessory ampulla. Gastroenterology 1981;81(6):1104-1110.
|
| 15. |
Bernard JP, Sahel J, Giovannini M, Sarles H. Pancreas divisum is a probable cause of acute pancreatitis: a report of 137 cases. Pancreas 1990;5(3):248-254.
|
| 16. |
Mariani A, Di Leo M, Petrone MC, et al. Outcome of endotherapy for pancreas divisum in patients with acute recurrent pancreatitis. World J Gastroenterol 2014;20(46):17468-17475.
|
| 17. |
Hayashi TY, Gonoi W, Yoshikawa T, et al. Ansa pancreatica as a predisposing factor for recurrent acute pancreatitis. World J Gastroenterol 2016;22(40):8940-8948.
|
| 18. |
Hać S, Nałęcz A, Dobosz M, et al. Pancreatic duct diversity. Pancreas 2009;38(3):318-21.
|
| 19. |
Bang S, Suh JH, Park BK, et al. The relationship of anatomic variation of pancreatic ductal system and pancreaticobiliary diseases. Yonsei Med. J 2006;47(2):243-248.
|
