

Does dietary advice combined with complete dentures improve the nutrient intake and nutritional status of edentulous patients? A systematic review with meta-analysis


Abstract
Background: The purpose of this systematic review and meta-analysis was to assess the nutrient intake and nutritional status of edentulous patients who received dietary advice combined with complete dentures.
Material and methods: Data were extracted from PubMed/Medline, Google Scholar, Scopus, and ScienceDirect from February 2002 to February 2025 by 2 independent reviewers. Ebscohost was searched for full-text articles from 1994 to 2025, in English. 1596 articles were excluded based on exclusion criteria and after removing 7 duplicates. Eight articles were included for qualitative analysis, followed by 3 articles for meta-analysis.
Results: Non-significant improvements were seen in the intake of calcium (p = 0.17), iron (p = 0.10), protein (p = 0.21) and vitamin D (p = 0.93). Heterogeneity was low, indicating consistent results. GRADE analysis indicated a low level of evidence.
Conclusions: Our results have not shown any significant improvement in nutrient intake after dietary advice and rehabilitation. In addition, the limited number of studies available for this meta-analysis highlights the need for more standardized, long-term clinical trials to achieve a higher level of evidence.
Citation
Rani S, Jain N, Gupta S, Kaur B, Bhatia K. Does dietary advice combined with complete dentures improve the nutrient intake and nutritional status of edentulous patients? A systematic review with meta-analysis. Eur J Transl Clin Med.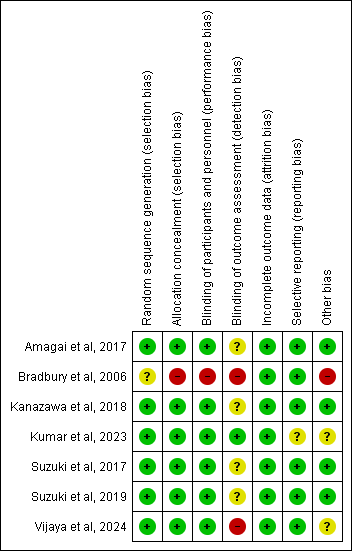














Introduction
The loss of teeth (edentulism) is considered an indication of poor oral cavity health [1-2]. Adequate nutrition is vital in maintaining a healthy life, especially in geriatric patients with complete removable prostheses [3]. Chen et al. reported that an estimated 0.35 billion people were affected by edentulism, accounting for 4.44% of the whole population [4]. This trend first increased in developed countries (e.g. UK and Japan) and later in developing countries such as India [5]. Literature has shown that dental status is closely linked to an individual’s nutritional status. Hence, for improved human health, dentition status should be monitored for nutritional counselling, particularly in the elderly [6].
Diet and nutrition are often misunderstood as synonyms, but they differ in that diet constitutes the ingestion of food, whereast nutrition integrates macro and micronutrients for the building and repairing of tissues [7]. The European Society for Clinical Nutrition and Metabolism recommends 1.0-1.2 g/kg body weight/day for healthy older adults and 1.2-1.5 g/kg/day for older adults who are malnourished or have a chronic illness [8]. The nutritional status of elderly people is often impaired due to selective food intake, as they are more comfortable with certain food items that are easy to chew with their current prostheses [9]. In addition to this, elderly patients often swallow inadequately chewed food as a compensatory mechanism for reduced masticatory efficiency, which may also indirectly contribute to nutritional deficiencies.
Evidence from the literature shows that edentulism is associated with a high risk of malnutrition [10-11]. In developed countries, adults aged 60 years or older without functional dentition were found to be at a higher risk of malnutrition compared to those with functional dentition [10]. Authors also emphasized the importance of using validated tools to determine malnutrition in the elderly population. In two systematic reviews, nutritional assessment was measured using the Mini Nutritional Assessment (MNA) or its short form (MNA-SF) [10-11]. In another systematic review, McGowan et al. examined the nutritional status of adults after prosthetic rehabilitation (dentures) combined with dietary advice, dietary outcomes, as assessed by the Brief-Type Self-Administered Diet History Questionnaire (BDHQ), and serum marker levels reported in analyzed studies [12].
Several studies have demonstrated that tooth loss is associated with a reduced intake of fruits and vegetables, as well as proteins and dietary fiber [13-14]. Previous research by Hamada et al. and Moynihan et al. have shown that prosthetic rehabilitation alone leads to less predictable positive dietary behavior change [15-16]. The evidence remains inconclusive regarding whether complete rehabilitation of functional dentition alone leads to significant improvement in overall nutritional status. Additionally, the combined effect of removable complete dentures and dietary counseling was not comprehensively assessed in completely edentulous patients. Hence, we conducted a systematic review with meta-analysis in order to synthesize the data on the improvement in nutrient intake and nutritional status of patients who received dietary advice combined with complete removable dentures.
Material and methods
Review design and registration
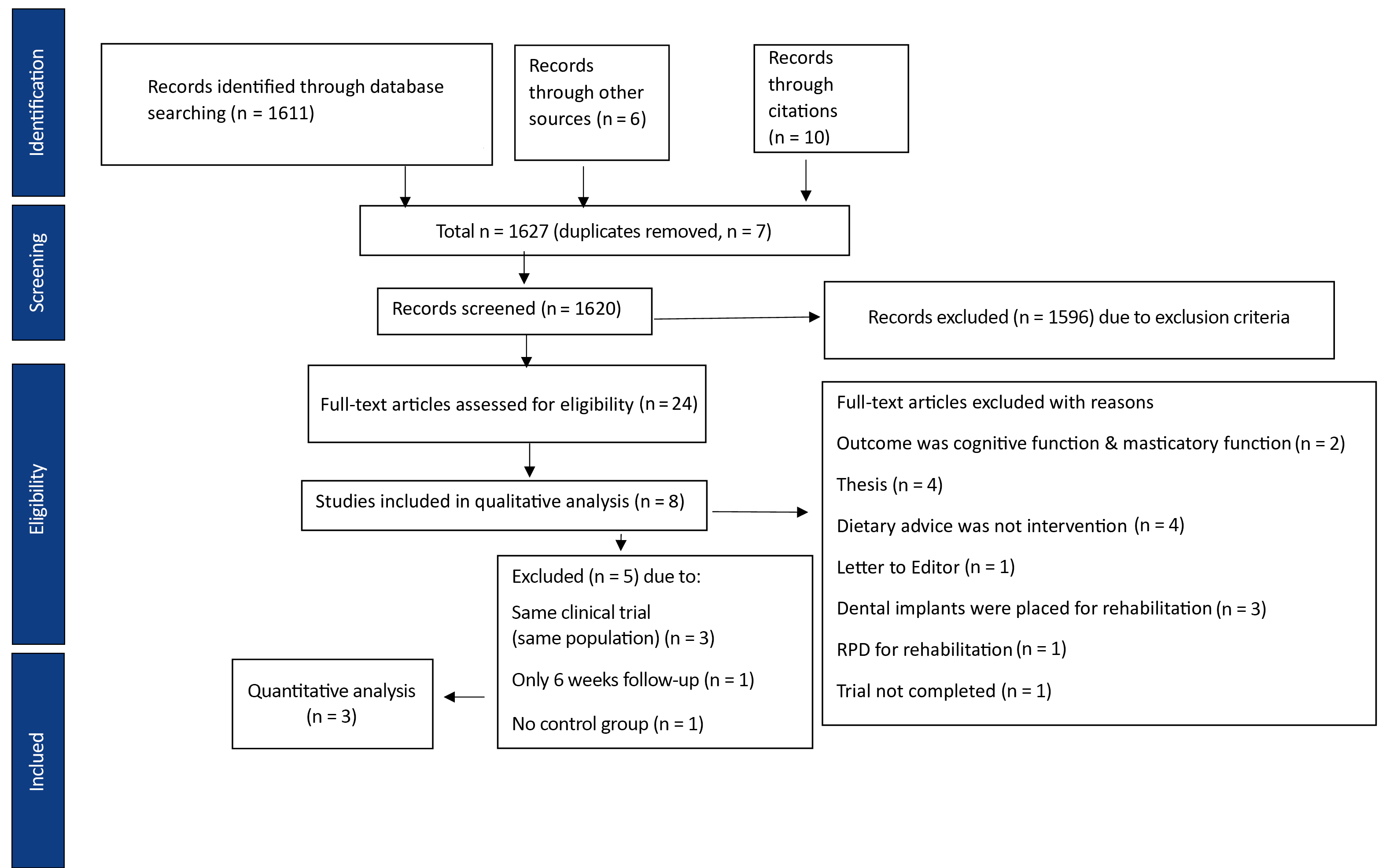
This review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) checklist (2020) and the Cochrane Handbook for Systematic Reviews and Meta-analysis [17-18]. The PRISMA flowchart is shown in Figure 1. Our systematic review was registered in PROSPERO (registration number CRD42025633956) on January 4, 2025. Data extraction was updated in PROSPERO on 1st March 2025.
Figure 1. PRISMA flowchart of our systematic review
Research question and PICOS
The research question for this systematic review was: “does supplemental dietary advice along with complete rehabilitation enhance nutrient intake and nutritional status for completely edentulous patients?” The studied population consisted of completely edentulous patients with removable complete dentures. The intervention involved supplementary dietary advice in any form for individuals with complete dentures. Control involved rehabilitation with complete dentures without dietary advice. The outcome measured was nutrient intake and nutritional status. We included full-text randomized clinical trials (RCTs), observational studies, and prospective clinical studies published in the English language. Exclusion criteria were: studies in which implant rehabilitation or partial rehabilitation was performed (the research question focused on complete denture therapy as the sole prosthetic rehabilitation), cross-sectional studies, case reports, theses, dissertations, pilot studies, studies published not in the English language, and unpublished data. Gray literature was not searched in this review.
Data extraction
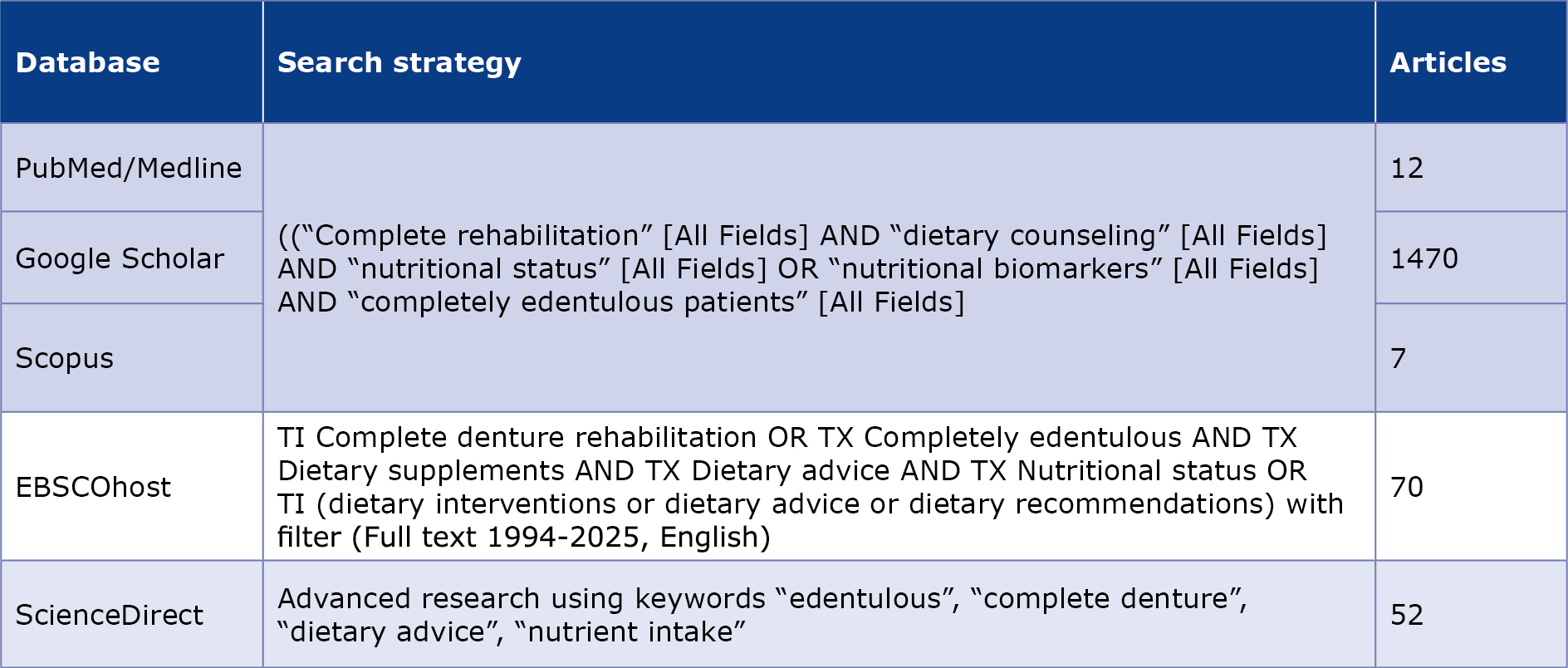
Two authors (SR and NJ) independently extracted data from PubMed/Medline (as of April 2, 2025), Google Scholar (as of February 24, 2025), Scopus (as of February 10, 2025), and ScienceDirect (as of February 22, 2025), covering the period from February 2002 to February 2025. Ebscohost (as of February 7, 2025) was searched using a filter for full text, covering the years 1994-2025, in English. The search strategy for individual databases is presented in Table 1.
Table 1. Search strategy used in this systematic review
Review outcomes
Our systematic review focused on assessing the nutritional status of completely edentulous patients post-intervention.
The nutrient intake was measured in terms of fruit and vegetable (F/V) intake, fiber, protein, fatty acids, energy, micronutrients, and macronutrients. At the same time, nutritional status was assessed using established questionnaires (MNA, MNA-SF, BDHQ) for the same or subsequent measurement of biochemical markers.
Meta-analysis
Two authors (SR and NJ) independently extracted data into a spreadsheet, detailing the authors, year of publication, country, demographic data, intervention details, and results at various time intervals. A meta-analysis was conducted using fixed-effects models to pool the quantitative data on patient nutrient intake, incorporating the mean and standard deviation values provided in the studies (Review Manager (Rev Man), v 5.4, Cochrane Collaboration). I2 statistics were used to calculate the heterogeneity.
Risk of bias
The Cochrane tool was used to assess the risk of bias (RoB), including domains selection bias, performance bias, detection bias, attrition bias, reporting bias, and other bias. A revised JBI RoB tool was used for observational studies [19]. Two independent reviewers reported RoB for all included studies under the high-risk, low-risk, or unclear-risk categories.
Level of evidence
The level of evidence was calculated using theGRADEpro GDT software (Evidence Prime Sp. z o.o., Kraków, Poland, available from gradepro.org). The quality was assessed as high, moderate, low or very low based on 5 criteria (risk of bias, inconsistency, indirectness, imprecision, other considerations).
Results
Search results
A total of 1611 articles were retrieved from the database search: 12 articles in PubMed, 1470 in Google Scholar, 70 in Ebscohost, 7 in Scopus and 52 in ScienceDirect. A manual search of the included articles’ reference lists identified 10 additional articles. 6 additional articles were selected from other sources (e.g., data registries, journals not indexed in databases). Google Scholar data was searched using MeSH keywords with Boolean operators AND and OR. Duplicates were removed manually by two independent reviewers (no software was used for removing duplicates in any database) (Table 1).
After removing 7 duplicates, the titles and abstracts were reviewed and 1596 articles were excluded based on the criteria listed earlier. If there was any confusion about an article, then the full text was read independently by 2 authors (SG and BK). To clarify any discrepancies regarding the inclusion of an article, a third reviewer was consulted until a clear consensus was reached. A total of 24 articles were assessed for eligibility and 8 were included for qualitative analysis (Figure 1). After excluding 5 more articles, 3 articles were included in the meta-analysis. In the event of any ambiguity, the decision was made by a third author (SR).
Included studies
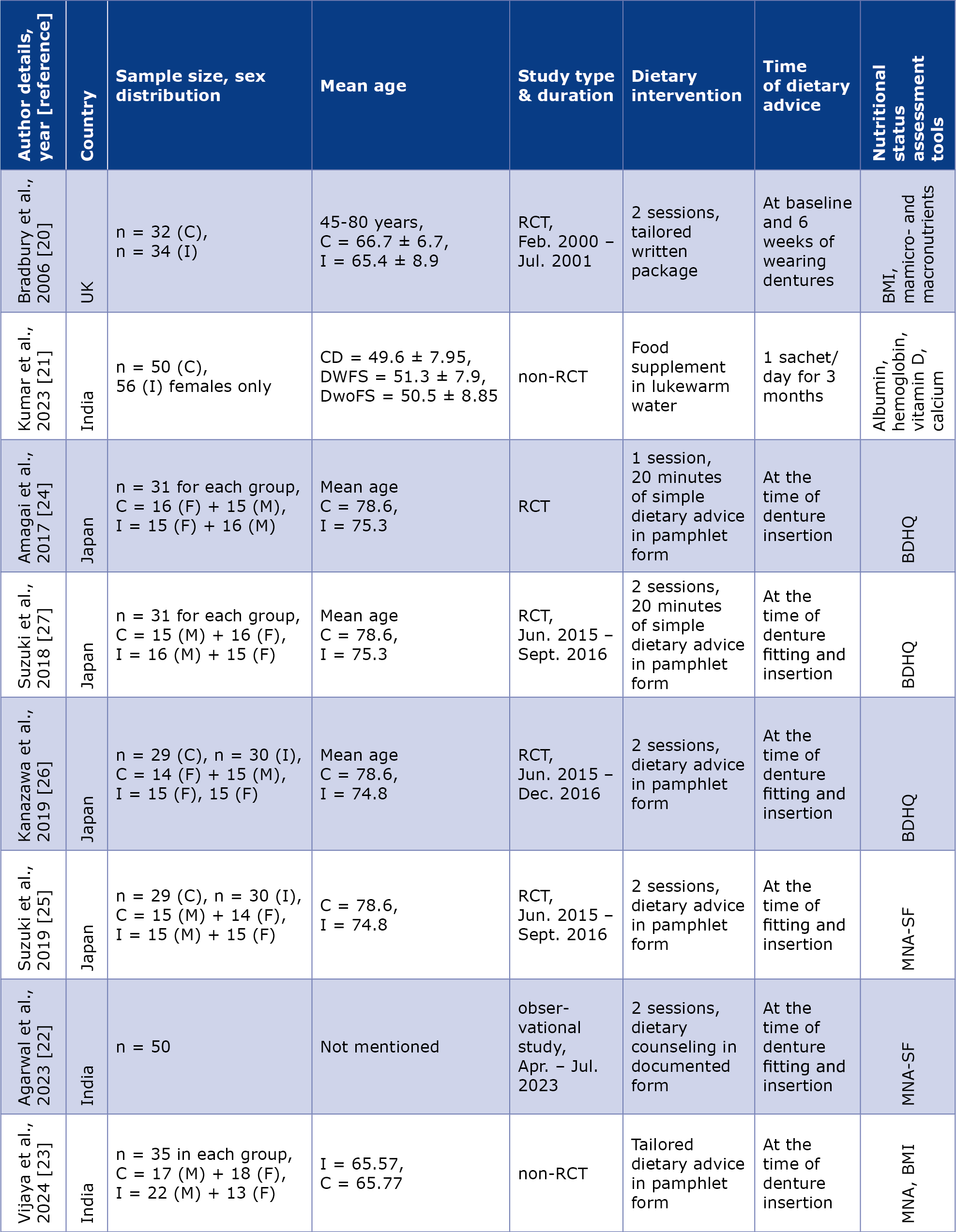
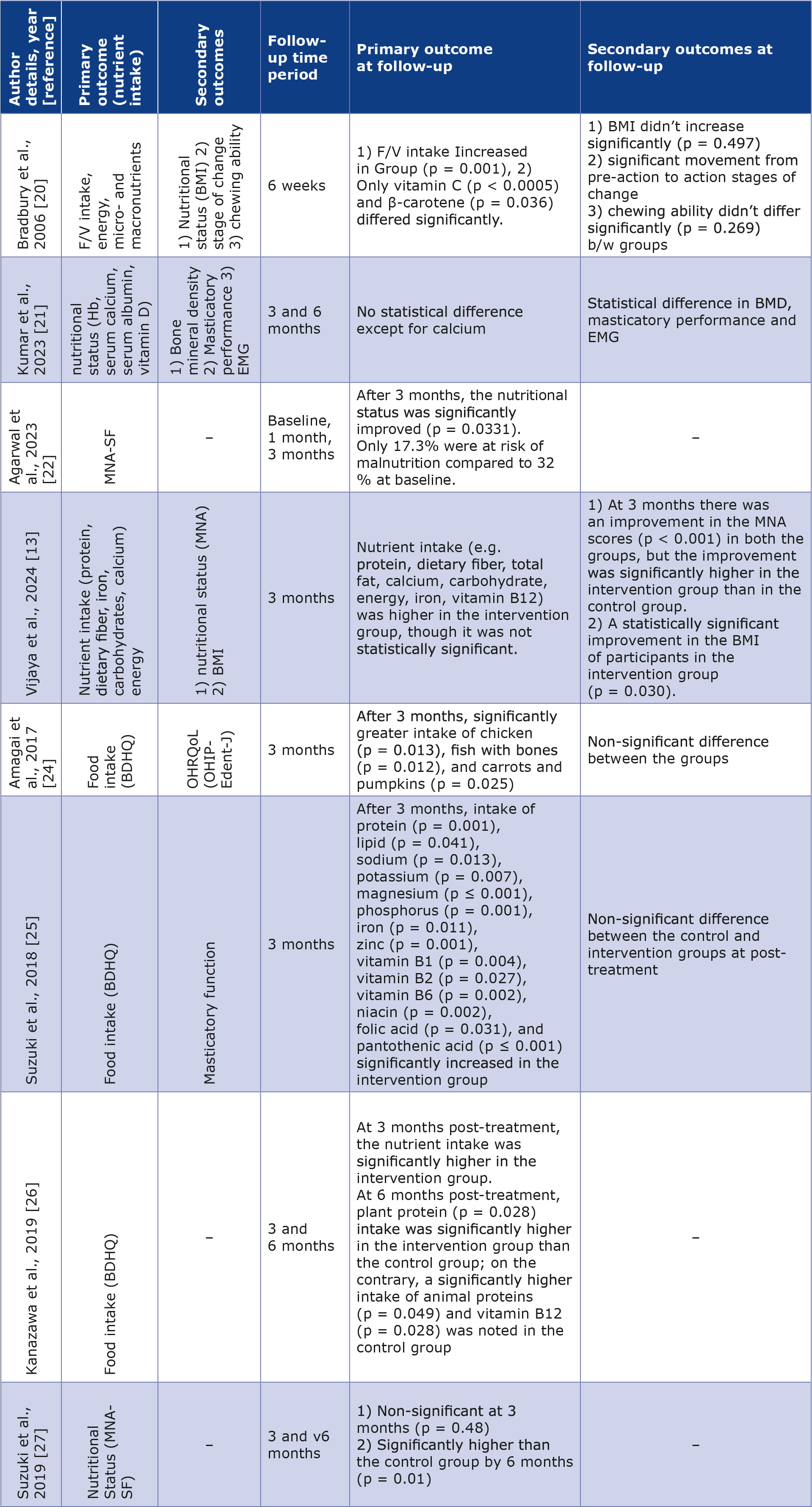
A total of 7 RCTs and 1 observational study were included for systematic review; 1 study was conducted in the UK [20], 3 in India [21-23] and 4 in Japan [24-27]. In one of the studies (Kumar et al.) all of the participants were female [21]. Ethical approval and informed consent were reported in all of the analysed trials. In most of the included studies, dietary advice was provided to the patients in the form of written pamphlets either at the time of fitting or insertion of dentures [20, 22-27]. An exception is the study by Kumar et al., in which patients received dietary advice in the form of food supplements for 3 months [21]. The Brief Self-Administered Diet History Questionnaire (BDHQ) was used to assess the nutritional status of patients in 3 studies [24-26]. In 1 study the MNA tool was used to determine the participants’ nourishment [23], while its short version (MNA-SF) was used in 2 others [22, 27]. Serum biomarkers (e.g. Vit D, Hb, serum Ca, BMI, BMD) were analysed in 3 studies [20-21, 23]. Masticatory performance was assessed in 2 studies [21, 25], 1 study also evaluated muscle activity using EMG [21] and one study assessed oral health-related quality of life [24] as secondary outcomes (Table 2). Baseline and follow-up mean values (along with standard deviation) for all included studies are provided in the Supplementary Table 1. The minimum follow-up time period in the included studies was 6 weeks, and the maximum follow-up period was 6 months. A summary of outcomes at different time periods is provided in Table 3.
Table 2. Partcipant demographics and dietary advice described in the included studies
BDHQ – Brief-Type Self-Administered Diet History Questionnaire, BMI – body mass index, C – control group, CD – completely dentate, DWFS – complete dentures without food supplement, DwoFS – complete dentures without food supplement, F – female, I – intervention group, M – male, MNA – Mini Nutritional Assessment, MNA-SF – Mini Nutritional Assessment-Short Form, non-RCT – non-randomized controlled trial, RCT – randomized controlled trial
Table 3. Outcome assessment of included studies
BDHQ – Brief-Type Self-Administered Diet History Questionnaire, BMD – bone mineral density, BMI – body mass index, EMG – electromyography, F/V – food and vegetable intake, Hb – hemoglobin, MNA – Mini Nutritional Assessment, MNA-SF – Mini Nutritional Assessment-Short Form, OHIP-Edent-J – Oral Health Impact Profile for Edentulous Patients (Japanese version), OHRQoL – Oral-health-related quality of life
Bias assessment
According to Cochrane’s tool for risk of bias assessment of RCTs, 6 of the included RCTs showed a low risk of bias and only one study had a high risk of bias [20]. Randomization and concealment of allocation were done adequately in 6 of the included studies. Reporting bias was also reduced by incorporating the appropriate measurement tool. In contrast, detection bias was high in 2 studies and unclear in 4 studies. The risk of bias in the 7 included RCTs is summarized in Figure 2. One of the included studies was observational and was found to have a low risk of bias, as calculated using the revised JBI tool [23].
Figure 2. Risk of bias graph of the included RCTs using the Cochrane tool
Meta-analysis
It was not possible to conduct a meta-analysis of nutritional status because 1 of the studies in which the MNA-SF was used was an observational study with no control group of participants [22].
A qualitative analysis was conducted on a total of 8 studies, and a further quantitative analysis was performed on 3 of these studies for nutrient intake. We included 4 different articles published from the same single clinical trial, featuring a different outcome measure in one of the studies and differences in the follow-up [24-27]. To avoid double-counting data or introducing bias, in the meta-analysis, , the same population with the same outcomes was considered only once across those 4 articles from the same clinical trial.
In the comparison of nutritional intake after a 3-month follow-up, 3 studies were included in the meta-analysis [21, 23, 26]. The heterogeneity across studies for the outcome ‘calcium intake’ was low (44%), so a fixed-effects model was used for analysis (Figure 3). The mean difference between the groups was -0.25 (95% confidence interval: -0.61 to 0.11). The pooled estimate did not show statistically significant differences (p = 0.17) in calcium intake between the intervention and control groups and the overall effect across studies showed results favouring the intervention group. Thus, it can be concluded that the mean calcium intake was better in the supplement group across all studies, although that difference was not statistically significant.
Figure 3. Forest plot distribution showing an outcome (calcium intake) with fixed effect model and 95% confidence interval
For the outcome ‘iron intake’ the heterogeneity across the analysed studies was low (0%), so a fixed-effects model was used for analysis (Figure 4). The mean difference between the groups was 1.16 (95% confidence interval: -0.21 to 2.54). The pooled estimate did not show statistically significant differences (p-value = 0.10) in iron intake between the intervention and control groups and the overall effect across studies showed results favouring the control group. Thus, it can be concluded that the mean iron intake was not (statistically) significant different between the two groups, however in clinical terms the control group showed comparable results to the intervention group.
Figure 4. Forest plot distribution showing an outcome (iron intake) with fixed effect model and 95% confidence interval
The heterogeneity across studies for the outcome ‘protein intake’ was low (0%), so a fixed-effects model was also used for analysis (Figure 5). The mean difference between the groups was 7.48 (95% confidence interval: -4.25 to 19.21). The pooled estimate showed no statistically significant differences (p-value = 0.21) in protein intake between the intervention and control groups, and the overall effect across studies showed results favouring the control group. Thus, it can be concluded that the mean protein intake was not (statistically) significantly different between the two groups, although clinically the control group showed comparable results to the test group.
Figure 5. Forest plot distribution showing an outcome (protein intake) with fixed effect model and 95% confidence interval
In terms of the outcome ‘vitamin D intake’, the heterogeneity across studies was low (0%), so a fixed-effects model was used for analysis (Figure 6). The mean difference between the groups was 0.01 (95% confidence interval: -0.23 to 0.25). The pooled estimate showed no statistically significant differences (p-value = 0.93) in vitamin D intake between the intervention and control groups, and the overall effect across studies showed results favoring both the intervention and control groups. Thus, it can be concluded that the mean vitamin D intake was similar results in the intervention and control groups. Publication bias was not assessed as only 3 studies were included in the meta-analysis.
Figure 6. Forest plot distribution showing an outcome (vitamin D intake) with fixed effect model and 95% confidence interval
GRADE analysis
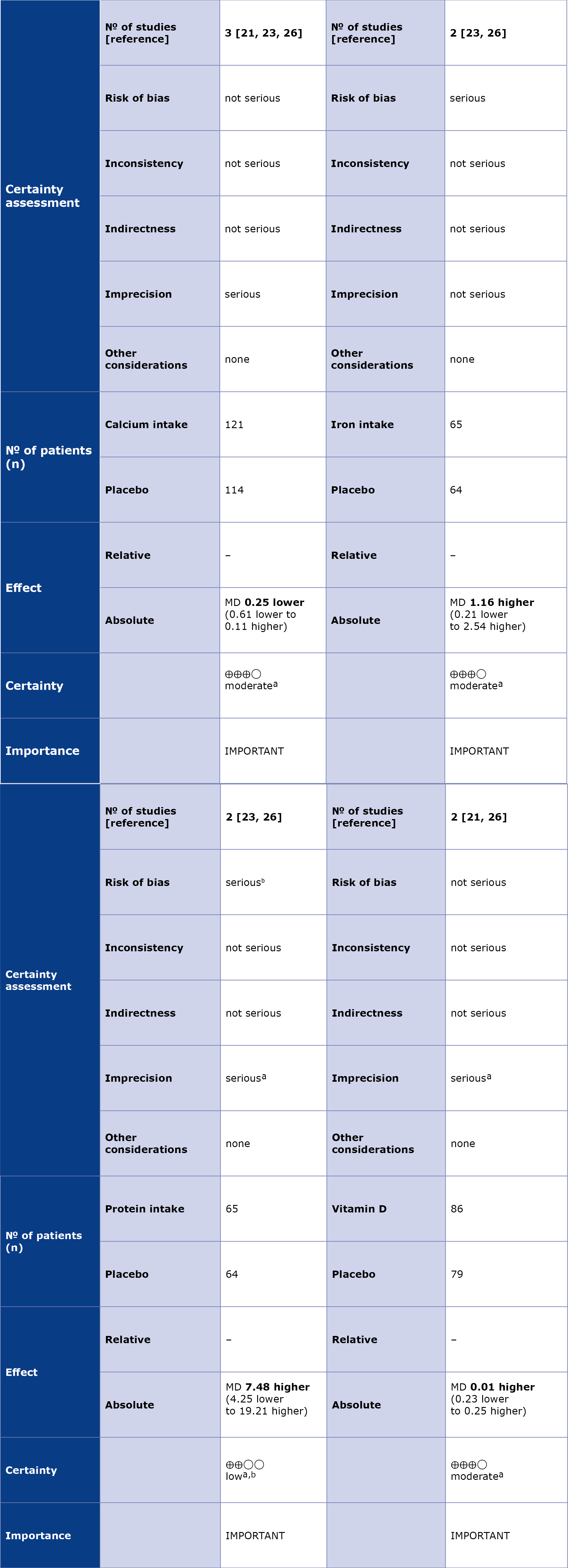
According to GRADE, there was a low level of evidence for the outcomes of ‘calcium intake’, ‘iron intake’, ‘protein intake’, and ‘vitamin D intake’, respectively. The evidence was downgraded considering 2 domains: risk of bias and imprecision. One of the included RCTs was of high risk, whereas the other 2 studies showed low risk. Imprecision among the studies was also graded as serious, considering the wide uncertainty surrounding the estimates and the crossing of decision thresholds (Table 4).
Table 4. Level of evidence assessed using the GRADE method
a – wide uncertainty around the estimate and crossing decision thresholds, b – high risk of bias, CI – confidence interval, MD – mean difference
Discussion
Complete tooth loss is directly related to dietary intake and nutritional status of individuals [28]. Completely edentulous patients with less functional occlusion tend to consume fewer fruits and vegetables and, hence, are more prone to systemic diseases [29-30]. In their systematic review, Hussein et al. indicated that people > 60 years of age who experience complete tooth loss face a 21% chance of malnutrition [11]. In another systematic review, the risk of malnutrition was found to be high in individuals who were partially/fully edentulous [12]. Findings from an umbrella review demonstrated that tooth loss (partial or complete) is a significant risk factor for malnutrition, indicating that compromised oral health can negatively impact nutritional status [31]. Although the above-cited systematic reviews demonstrated an association between nutritional status and the elderly population, we did not find a comprehensive review regarding the completely edentulous patients.
People with tooth loss tend to avoid chewing raw fruits and vegetables, which reduces their intake of protein and fiber, leading to low energy levels. Rehabilitation of functional units with complete dentures can empower patients to maintain a healthy nutrient intake [32]. However, studies have also shown that prosthetic rehabilitation alone may not be sufficient to enhance nutritional status [27, 33]. Simple dietary advice, supplemented with comprehensive rehabilitation, has been proven as an effective way to improve the nutritional outcomes of patients [25, 28].
Dietary advice can be provided in various forms (e.g. written pamphlets, individual consultations, tailored dietary regimens or specified food supplements), all of which can be customized according to age, sex, and individual requirements. However, providing tailored diet plans for patients in a dental setting is difficult as dentists lack specific knowledge of dietary supplements. Hence, in most of the included studies, simple dietary advice was provided to participants in written pamphlet form [22, 24-27].
There are various standardized tools for assessing nutritional status, while nutrient intake is evaluated through different components, including macronutrients and micronutrient intake. In our systematic review, the BDHQ questionnaire was administered in 3 studies [24-26]. Although the BDHQ is short (4 pages, can be completed in 10-15 minutes) and easy to understand, the drawback of this tool is that answers depend on the patients’ recall of key details (e.g. the food they consumed, diet preparation, intake of beverages, including alcohol). This may result in recall bias during assessment of elderly participants.
A few studies measured components of fruit and vegetable intake, macronutrients, and micronutrients after intervention [20, 23-26]. In our review, it was found that the nutrient intake of calcium, iron, protein, and vitamin D was slightly improved after dietary advice, although the difference was non-significant. Our results were not consistent with other studies, as in a clinical trial conducted by Kanazawa et al., the intake of protein (p = 0.004), iron (p = 0.035) was statisticaly significant, but calcium (p = 0.281) and vitamin D (p = 0.295) were not statistically significant in the intervention group after 3 months of follow-up [26]. In a study by Vijaya et al., the intervention group showed no statistically significant differences in protein (p = 0.30) or calcium intake (p = 0.196) after the same follow-up period [23]. In contrast, Kumar et al. found that calcium intake was significantly higher with supplements (p = 0.01), but not with vitamin D (p = 0.30). The differences in these results may be due to variations in the demographic distributions of the populations, as 1 of the analysed studies was conducted in Japan and the other 2 in India. Another variation was the exclusion of male participants in one of the analysed studies [23].
In their meta-analysis Bezerra et al. concluded that in completely edentulous patients the bioavailability of the nutrients remained stable with implant-supported dentures. They also emphasized the role of the nutritional specialist for the outcomes of rehabilitation [34]. Additionally, nutrient intake is influenced by multiple factors, particularly in edentulous patients, therefore the systemic health condition of the included population in trials should be taken into consideration. The meta-analysis also reveals low heterogeneity, as indicated by the forest plots, with consistent results and a low level of evidence. In one of the analysed studies, Kumar et al. presented calcium and Vitamin D intake were presented as median and IQR [21]. By using the formula described by Wan et al., we converted these values into mean and SD for inclusion in our meta-analysis [35].
For, The MNA [23], MNA-SF [22, 27], or more informative assessments, such as BMI [20, 23], and serum biomarkers (Hb, Ca, Fe) [21], have been used by the authors for assessment of the participants’ nutritional status in the included studies. The MNA-SF determines the population at risk of malnutrition via only 6 questions, compared to the MNA form which includes screening followed by a detailed assessment. In a study, after a 3-month follow-up, nutrient intake was significantly better in the intervention group (p = 0.0331) [22], compared to another study in which significant improvement was found after 6 months (p = 0.01) [25]. Vijaya et al. reported that MNA scores were significantly improved in both the control and intervention groups after 3 months (p < 0.001), while there was only a slight improvement in the intervention group when inter-group comparison was carried out [23]. This result was supported by a more reliable marker (BMI), which significantly improved in that study’s intervention group [23].
A limitation of our analysis is that most of the included studies were conducted in Japan, India, and the UK, therefore the dietary advice provided in these studies cannot be generalized to other populations. The dietary advice was limited to only 1 or 2 consultations during the study period. There was a paucity of literature on the assessment of nutritional status using the same tool for meta-analysis with a long follow-up. More RCTs are needed using a standard tool to determine the nutrient intake and nutritional status of edentulous patients when supplemented with dietary advice and complete denture therapy. Long-term follow-up and regular reinforcement of dietary advice are required in future studies to assess whether the outcomes are due to prostheses or dietary advice.
Conclusions
Within the limitations of our analysis, it can be concluded that there was no significant difference in the nutrient intake of calcium, iron, protein, and vitamin D in people who received dietary advice along with complete dentures. Furthermore, nutritional status was improved in the intervention group, but additional standardized long-term RCTs are required to obtain conclusive results.
Funding
Self funded.
Conflict of interest
None.
References
| 1. |
Chalub LLFH, Ferreira RC, Vargas AMD. Influence of functional dentition on satisfaction with oral health and impacts on daily performance among Brazilian adults: a population-based cross-sectional study. BMC Oral Health [Internet]. 2017;17(1):112. Available from: http://bmcoralhealth.biomedcentral.com/articles/10.1186/s12903-017-0402-5.
|
| 2. |
Lamster IB, Asadourian L, Del Carmen T, Friedman PK. The aging mouth: differentiating normal aging from disease. Periodontol 2000 [Internet]. 2016;72(1):96–107. Available from: https://onlinelibrary.wiley.com/doi/10.1111/prd.12131.
|
| 3. |
Kazemi S, Savabi G, Khazaei S, Savabi O, Esmaillzadeh A, Keshteli AH, et al. Association between food intake and oral health in elderly: SEPAHAN systematic review no. 8. Dent Res J (Isfahan) [Internet]. 2011;8(Suppl 1):S15-20. Available from: http://www.ncbi.nlm.nih.gov/pubmed/23372590.
|
| 4. |
Chen HM, Shen K, Ji L, McGrath C, Chen H. Global and Regional Patterns in Edentulism (1990-2021) With Predictions to 2040. Int Dent J [Internet]. 2025;75(2):735–43. Available from: https://www.sciencedirect.com/science/article/pii/S0020653924016162.
|
| 5. |
Noto S. Perspectives on Aging and Quality of Life. Healthcare [Internet]. 2023;11(15):2131. Available from: https://www.mdpi.com/2227-9032/11/15/2131.
|
| 6. |
Sahyoun NR, Lin C-L, Krall E. Nutritional status of the older adult is associated with dentition status. J Am Diet Assoc [Internet]. 2003;103(1):61–6. Available from: https://linkinghub.elsevier.com/retrieve/pii/S000282230200007X.
|
| 7. |
Perry C. Nutrition for senescent denture patients. J Prosthet Dent [Internet]. 1961;11(1):73–8. Available from: https://linkinghub.elsevier.com/retrieve/pii/0022391361901123.
|
| 8. |
Deutz NEP, Bauer JM, Barazzoni R, Biolo G, Boirie Y, Bosy-Westphal A, et al. Protein intake and exercise for optimal muscle function with aging: Recommendations from the ESPEN Expert Group. Clin Nutr [Internet]. 2014;33(6):929–36. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0261561414001113.
|
| 9. |
Joshipura KJ, Willett WC, Douglass CW. The impact of edentulousness on food and nutrient intake. J Am Dent Assoc [Internet]. 1996;127(4):459–67. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0002817715613939.
|
| 10. |
Zelig R., Goldstein S., Touger-Decker R., Firestone E., Golden A., Johnson Z., et al. Tooth Loss and Nutritional Status in Older Adults: A Systematic Review and Meta-analysis. JDR Clin Transl Res [Internet]. 2022;7(1):4–15. Available from: https://doi.org/10.1177/2380084420981016.
|
| 11. |
Hussein S, Kantawalla RF, Dickie S, Suarez-Durall P, Enciso R, Mulligan R. Association of Oral Health and Mini Nutritional Assessment in Older Adults: A Systematic Review with Meta-analyses. J Prosthodont Res [Internet]. 2022;66(2):JPR_D_20_00207. Available from: https://www.jstage.jst.go.jp/article/jpr/66/2/66_JPR_D_20_00207/_article.
|
| 12. |
McGowan L, McCrum L-A, Watson S, Cardwell C, McGuinness B, Rutherford H, et al. The impact of oral rehabilitation coupled with healthy dietary advice on the nutritional status of adults: A systematic review and meta-analysis. Crit Rev Food Sci Nutr [Internet]. 2020;60(13):2127–47. Available from: https://www.tandfonline.com/doi/full/10.1080/10408398.2019.1630600.
|
| 13. |
Nakamura M, Ojima T, Nagahata T, Kondo I, Ninomiya T, Yoshita K, et al. Having few remaining teeth is associated with a low nutrient intake and low serum albumin levels in middle-aged and older Japanese individuals: findings from the NIPPON DATA2010. Environ Health Prev Med [Internet]. 2019;24(1):1. Available from: https://environhealthprevmed.biomedcentral.com/articles/10.1186/s12199-018-0752-x.
|
| 14. |
Iwasaki M, Yoshihara A, Ogawa H, Sato M, Muramatsu K, Watanabe R, et al. Longitudinal association of dentition status with dietary intake in Japanese adults aged 75 to 80 years. J Oral Rehabil [Internet]. 2016;43(10):737–44. Available from: https://onlinelibrary.wiley.com/doi/10.1111/joor.12427.
|
| 15. |
Hamada MO, Garrett NR, Roumanas ED, Kapur KK, Freymiller E, Han T, et al. A randomized clinical trial comparing the efficacy of mandibular implant-supported overdentures and conventional dentures in diabetic patients. Part IV: Comparisons of dietary intake. J Prosthet Dent [Internet]. 2001;85(1):53–60. Available from: https://www.sciencedirect.com/science/article/pii/S0022391301634589.
|
| 16. |
Moynihan P., Butler T., Thomason J., Jepson NJ. Nutrient intake in partially dentate patients: the effect of prosthetic rehabilitation. J Dent [Internet]. 2000;28(8):557–63. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0300571200000440.
|
| 17. |
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ [Internet]. 2021;n71. Available from: https://www.bmj.com/lookup/doi/10.1136/bmj.n71.
|
| 18. |
Higgins J, Thomas J. Cochrane handbook for systematic reviews of interventions [Internet]. 6.5. Cochrane. 2024 [cited 2026 May 22]. Available from: https://www.cochrane.org/authors/handbooks-and-manuals/handbook.
|
| 19. |
Barker TH, Habibi N, Aromataris E, Stone JC, Leonardi-Bee J, Sears K, et al. The revised JBI critical appraisal tool for the assessment of risk of bias for quasi-experimental studies. JBI Evid Synth [Internet]. 2024;22(3). Available from: https://journals.lww.com/jbisrir/fulltext/2024/03000/the_revised_jbi_critical_appraisal_tool_for_the.4.aspx.
|
| 20. |
Bradbury J, Thomason JM, Jepson NJA, Walls AWG, Allen PF, Moynihan PJ. Nutrition Counseling Increases Fruit and Vegetable Intake in the Edentulous. J Dent Res [Internet]. 2006;85(5):463–8. Available from: https://journals.sagepub.com/doi/10.1177/154405910608500513.
|
| 21. |
Kumar K, Kumar S, Khandpur M, Singh N, Singh BP, Garg RK. The effect of food supplements on completely edentulous women rehabilitated with complete dentures: A randomized controlled trial. J Indian Prosthodont Soc [Internet]. 2023;23(4):347–55. Available from: https://journals.lww.com/10.4103/jips.jips_237_23.
|
| 22. |
Agrawal S, Sathe S, Paul P, Doshi K, Agrawal A, Rathi N. Evaluation of the Role of Dentures & Dietary Advice on Nutritional Status of Complete Edentulous Patients Using MNA®-SF: An Observational Study. Cureus [Internet]. 2023; Available from: https://www.cureus.com/articles/196426-evaluation-of-the-role-of-dentures--dietary-advice-on-nutritional-status-of-complete-edentulous-patients-using-mna-sf-an-observational-study.
|
| 23. |
Vijaya S, Rodrigues A, Garg M, Vijaya S, Shetty MJ, Dhanania S. Effectiveness of dietary intervention in geriatric patients receiving new complete dentures: A randomized controlled trial. J Indian Prosthodont Soc [Internet]. 2024;24(4):329–35. Available from: https://journals.lww.com/10.4103/jips.jips_166_24.
|
| 24. |
Amagai N, Komagamine Y, Kanazawa M, Iwaki M, Jo A, Suzuki H, et al. The effect of prosthetic rehabilitation and simple dietary counseling on food intake and oral health related quality of life among the edentulous individuals: A randomized controlled trial. J Dent [Internet]. 2017;65:89–94. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0300571217301793.
|
| 25. |
Suzuki H, Kanazawa M, Komagamine Y, Iwaki M, Amagai N, Minakuchi S. Changes in the nutritional statuses of edentulous elderly patients after new denture fabrication with and without providing simple dietary advice. J Prosthodont Res [Internet]. 2019;63(3):288–92. Available from: https://linkinghub.elsevier.com/retrieve/pii/S188319581830152X.
|
| 26. |
Kanazawa M, Suzuki H, Komagamine Y, Iwaki M, Amagai N, Minakuchi S. Combined effects of new complete denture fabrication and simplified dietary advice on nutrient intake in edentulous elderly patients for 6 months. Clin Oral Investig [Internet]. 2019;23(5):2245–52. Available from: http://link.springer.com/10.1007/s00784-018-2669-6.
|
| 27. |
Suzuki H, Kanazawa M, Komagamine Y, Iwaki M, Jo A, Amagai N, et al. The effect of new complete denture fabrication and simplified dietary advice on nutrient intake and masticatory function of edentulous elderly: A randomized-controlled trial. Clin Nutr [Internet]. 2018;37(5):1441–7. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0261561417302637.
|
| 28. |
Yoshida M, Kikutani T, Yoshikawa M, Tsuga K, Kimura M, Akagawa Y. Correlation between dental and nutritional status in community‐dwelling elderly Japanese. Geriatr Gerontol Int [Internet]. 2011;11(3):315–9. Available from: https://onlinelibrary.wiley.com/doi/10.1111/j.1447-0594.2010.00688.x.
|
| 29. |
Crowe FL, Roddam AW, Key TJ, Appleby PN, Overvad K, Jakobsen MU, et al. Fruit and vegetable intake and mortality from ischaemic heart disease: results from the European Prospective Investigation into Cancer and Nutrition (EPIC)-Heart study. Eur Heart J [Internet]. 2011;32(10):1235–43. Available from: https://academic.oup.com/eurheartj/article-lookup/doi/10.1093/eurheartj/ehq465.
|
| 30. |
Li M, Fan Y, Zhang X, Hou W, Tang Z. Fruit and vegetable intake and risk of type 2 diabetes mellitus: meta-analysis of prospective cohort studies. BMJ Open [Internet]. 2014;4(11):e005497. Available from: http://dx.doi.org/10.1136/bmjopen-2014-005497.
|
| 31. |
Kaurani P, Kakodkar P, Bhowmick A, Samra RK, Bansal V. Association of tooth loss and nutritional status in adults: an overview of systematic reviews. BMC Oral Health [Internet]. 2024;24(1):838. Available from: https://bmcoralhealth.biomedcentral.com/articles/10.1186/s12903-024-04602-1.
|
| 32. |
Sysal P, Veronese N, Arik F, Kalan U, Smith L, ISIK AT. Mini Nutritional Assessment Scale-Short Form can be useful for frailty screening in older adults. Clin Interv Aging [Internet]. 2019;Volume 14:693–9. Available from: https://www.dovepress.com/mini-nutritional-assessment-scale-short-form-can-be-useful-for-frailty-peer-reviewed-article-CIA.
|
| 33. |
Brígido JA, de Oliveira da Rosa WL, Lund RG. The effect of prosthetic rehabilitation with or without dietary advice on nutritional status in elderly patients: a systematic review. Aging Clin Exp Res [Internet]. 2023;35(11):2399–411. Available from: https://link.springer.com/10.1007/s40520-023-02578-6.
|
| 34. |
Bezerra AP, Gama LT, Pereira LJ, van der Bilt A, Peyron M-A, Rodrigues Garcia RCM, et al. Do implant-supported prostheses affect bioavailability of nutrients of complete and partially edentulous patients? A systematic review with meta-analysis. Clin Nutr [Internet]. 2021;40(5):3235–49. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0261561421000923.
|
| 35. |
Wan X, Wang W, Liu J, Tong T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med Res Methodol [Internet]. 2014;14(1):135. Available from: https://bmcmedresmethodol.biomedcentral.com/articles/10.1186/1471-2288-14-135.
|
