


Endoscopic spine surgery: methodology and outcomes based on patient feedback


Abstract
Background: Endoscopic lumbar decompression (ELD) is emerging as a minimally invasive alternative to traditional microdiscectomy, potentially offering faster recovery and reduced tissue damage. Our aim was to analyze clinical outcomes following the introduction of single-port ELD at our institution.
Material and methods: A retrospective analysis of 28 consecutive patients undergoing single-port ELD (2019-2023) was conducted. Most surgeries involved the L5-S1 level (77.8%) and utilized a translaminar approach (85.7%). Primary outcomes included the Oswestry Disability Index (ODI) and Numerical Rating Scale (NRS) pain scores.
Results: Mean ODI improved significantly from 65.1% pre-operative to 15.1% post-operative (p < 0.0001). Mean NRS scores improved from 8.33 to 2.36 (p < 0.0001). A minimal clinically important difference (MCID) was achieved in 92.9% of patients. Intraoperative conversions to open surgery occurred in 10.7% of cases. Post-operative complications were observed in 10.7% of patients (2 instances of paresis and 1 recurrence), with one case requiring reoperation.
Conclusions: Single-port ELD yields substantial improvements in both functional outcomes and pain relief. However, moderate complication and conversion rates reflect the technical learning curve. Extended follow-up is required to assess long-term recurrence and durability.
Citation
Krakowiak M, Palus D K, Mundayadan V P, Myszkowska B M, Grochowski C, Kulesza B, Nadolska E, Sokal P. Endoscopic spine surgery: methodology and outcomes based on patient feedback. Eur J Transl Clin Med. 2026;9(1):59-65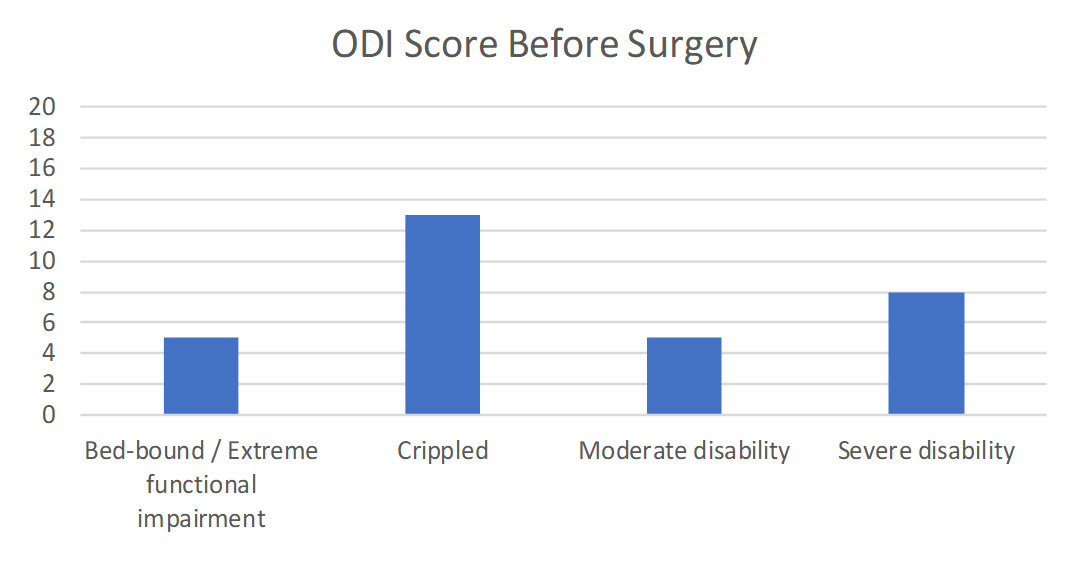










Introduction
Endoscopic lumbar decompression (ELD) has evolved considerably since Kambin and Gellman first described percutaneous lateral discectomy of the lumbar spine in 1983 [1]. Over the subsequent four decades, advances in optics, instrumentation, and surgical technique have transformed ELD from an experimental concept into a viable minimally invasive alternative to conventional open discectomy (OD) and microdiscectomy (MD) for the treatment of lumbar disc herniation and spinal stenosis [2-3]. Despite this progress, traditional techniques such as MD remain the predominant surgical method worldwide, as they are long-established and familiar to the majority of surgeons [4].
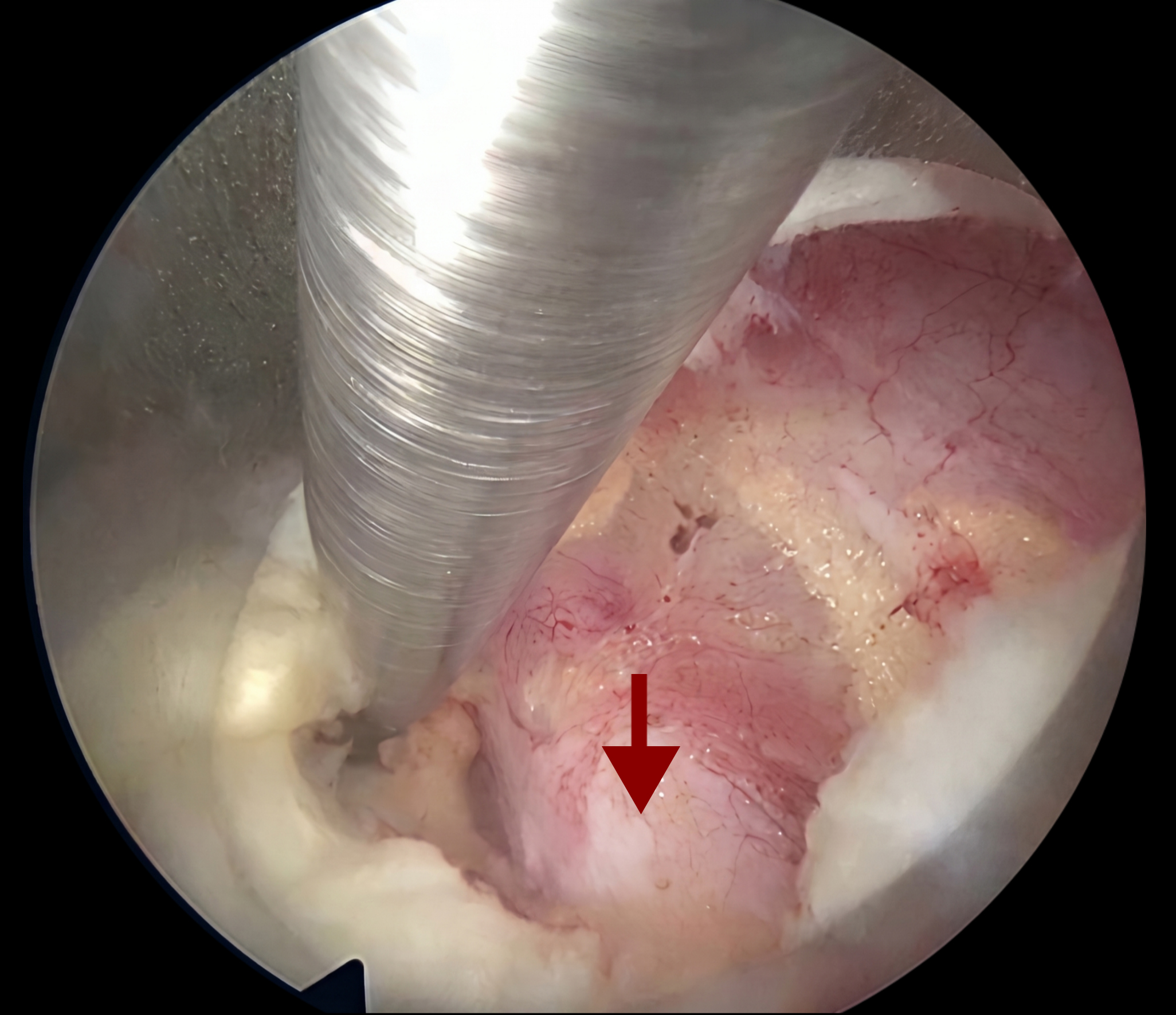
A growing body of evidence supports the benefits of ELD over conventional approaches. Comparative studies have demonstrated that ELD is associated with smaller incisions (often 10-16 mm), reduced paraspinal muscle disruption, less intraoperative blood loss, shorter operating times, and decreased post-operative pain compared to traditional microscopic discectomy [5-6]. These advantages lead to faster recovery, shorter hospital stays, and an earlier return to daily activities [7]. However, adoption of ELD remains limited due to the prolonged learning curve and the need for specialized instruments [3, 8]. For example, rigid endoscopy-assisted procedures require neurosurgeons to develop specialized skills for handling single-port endoscopes and adapting to two-dimensional video-guided navigation in confined surgical corridors (Figure 1) [9].
Figure 1. A compressed nerve root (red arrow) in the endoscopic view
Despite these challenges, the continued development of less invasive surgical techniques has driven interest in ELD as the preferred alternative to MD and OD [10]. In this retrospective study, we aimed to assess the surgical outcomes of ELD and patient-reported feedback following the adoption of this technique at our institution.
Materials and methods
Patient selection and demographics
We retrospectively analyzed 28 consecutive patients with complete pre-operative and post-operative outcome data who underwent single-port ELD between January 2019 and December 2023. These 28 patients were selected from a total of 40 endoscopic lumbar procedures performed at our institution during this period by 3 neurosurgeons in the early phases of acquiring endoscopic surgical expertise (< 100 cumulative endoscopic cases at study initiation).
The 28-patient cohort consisted of 14 males (50.0%) and 14 females (50.0%), with a mean age of 46.1 ± 8.8 years (range, 26-58 years). The following levels of the spine were operated: L5-S1 (n = 21, 77.8%), L4-L5 (n = 5, 18.5%), and L3-L4 (n = 1, 3.7%). One patient’s operative level was not recorded in the database and was excluded from level-specific analysis (n = 27 for level analysis).
Inclusion criteria
The patient inclusion criteria were: age (≥ 18 years at time of surgery), primary lumbar disc herniation confirmed on magnetic resonance imaging (MRI), lumbar spinal stenosis (with or without associated disc herniation) confirmed on MRI, radiculopathy or neurogenic claudication refractory to conservative management (≥ 6 weeks of non-operative treatment, including physical therapy and/or pharmacologic management), ODI score > 40% at baseline, sufficient cognitive and language capacity to independently complete standardized outcome questionnaires during the pre-operative and post-operative assessments.
Exclusion criteria
The exclusion criteria were: recurrent disc herniation at the same operative level, spinal instability (spondylolisthesis > Grade 1, spondylolysis with translation, or scoliosis > 20°), prior surgical intervention at the same spinal level as the one considered for endoscopic treatment, cauda equina syndrome presenting as an emergency requiring urgent decompression, severe systemic comorbidities (uncontrolled cardiac arrhythmia, severe pulmonary dysfunction, severe hepatic disease, uncontrolled diabetes), and active coagulopathy (or anticoagulation therapy that could not be safely discontinued perioperatively).
Anesthesia and positioning
Patients were positioned prone on a radiolucent operating table under general endotracheal anesthesia. Neuromonitoring (including transcranial motor evoked potentials (tcMEP) and somatosensory evoked potentials (SSEP)) was recorded from bilateral lower extremities to assess nerve root and spinal cord function throughout the procedure. Vital and peri-operative parameters (including continuous electrocardiography, pulse oximetry, end-tidal capnography and core temperature) were monitored in accordance with the American Society of Anesthesiologists (ASA) standards.
Surgical technique and operative parameters
All procedures utilized a single-port rigid endoscopic approach. A rigid 4-mm single-port endoscope with integrated visualization and bimanual working channels (Karl Storz SE & Co. KG, Tuttlingen, Germany) was connected to a high-definition video system and an appropriate illumination source. Surgeon preference, anatomical considerations, and the site of pathology determined the selection of surgical approach (transforaminal vs. translaminar). Four patients (14.3%) were operated via transforaminal approach, while the translaminar approach was chosen in 24 patients (85.7%).
Translaminar approach (n = 24)
Following skin sterilization, a small midline skin incision (approximately 10-16 mm) was made over the lumbodorsal (thoracolumbar) fascia at the affected spinal level under fluoroscopic guidance. The fascia was incised, and sequential dilation of the interlaminar space was performed using dilators. The endoscope was advanced into the interlaminar space, providing direct visualization of the ligamentum flavum, dura mater, nerve root, and any herniated disc material or osteophytes. Endoscopic decompression was achieved through the removal of ligamentous and osseous structures using endoscopic graspers, curettes, and a 3000 RPM endoscopic burr under direct visualization. Hemostasis was maintained using bipolar radiofrequency coagulation. Adequate decompression was confirmed by direct visualization of the nerve root and traversing dura without compression.
Transforaminal approach (n = 4)
Following fluoroscopic localization of the target foramen, a small lateral skin incision was made. Sequential dilators (6 mm and 8 mm) were used to dilate the intervertebral foramen through the paravertebral musculature under fluoroscopic guidance in a progressive manner. The endoscope was advanced through the dilators, permitting visualization of the foraminal anatomy, exiting nerve root, and any herniated disc material within the foramen or subarticular space. Endoscopic decompression involved the removal of disc material and osteophytes compressing the nerve root, followed by hemostasis with bipolar coagulation.
Intraoperative conversion
If adequate decompression could not be achieved via the endoscopic approach (due to technical factors or anatomical constraints), conversion to open microscopic or open surgical approach was planned and documented. Three patients (10.7%) underwent intraoperative conversion: 2 to open microscopic decompression and 1 to wide surgical decompression.
Follow-up assessment
Post-operative clinical assessments were conducted at standardized intervals: at post-operative week 2 (wound assessment), week 6 (clinical evaluation), week 12 (clinical and functional assessment), and at final follow-up (mean 4.5 months, range 3-6 months). Imaging included post-operative MRI at a mean of 6 weeks to assess adequacy of neural decompression, exclude recurrent or persistent herniation, and rule out complications.
Outcome measurement
Primary outcome measures
We used the Oswestry Disability Index (ODI) version 2.0, a 10-item condition-specific disability questionnaire that quantifies functional limitations attributable to low back pain [11]. Scores range from 0 to 100%, with higher scores indicating greater functional disability. Standard disability categories are defined as follows: 0-20% (minimal disability), 21- -40% (moderate disability), 41-60% (severe disability), 61-80% (very severe disability), and 81-100% (bedbound/extreme functional impairment).
To standardize the patients’ assessment of lower back and radicular pain intensity, we used the 11-point Numerical Rating Scale (NRS), ranging from 0 (no pain) to 10 (worst possible pain) [12]. The minimal clinically important difference (MCID) for NRS in lower extremity pain is generally considered to be ≥ 2.0 points [13].
The ODI and NRS questionnaires were administered in a structured format using a standardized script to minimize interviewer variability. Patients were asked to respond to each item independently without guidance or suggestion.
Secondary outcome measures
Secondary outcomes included: return to work status (percentage of patients returning to baseline occupation or equivalent duties), resumption of activities of daily living without significant limitation, and patient satisfaction with surgical outcome, (assessed using a 5-point Likert scale: very dissatisfied, dissatisfied, neutral, satisfied, very satisfied) [14]. Structured interviews were administered by trained research staff at baseline (pre-operatively) and at final follow-up (mean 4.5 months post-operatively).
Results
Primary outcome: disability (Oswestry Disability Index)
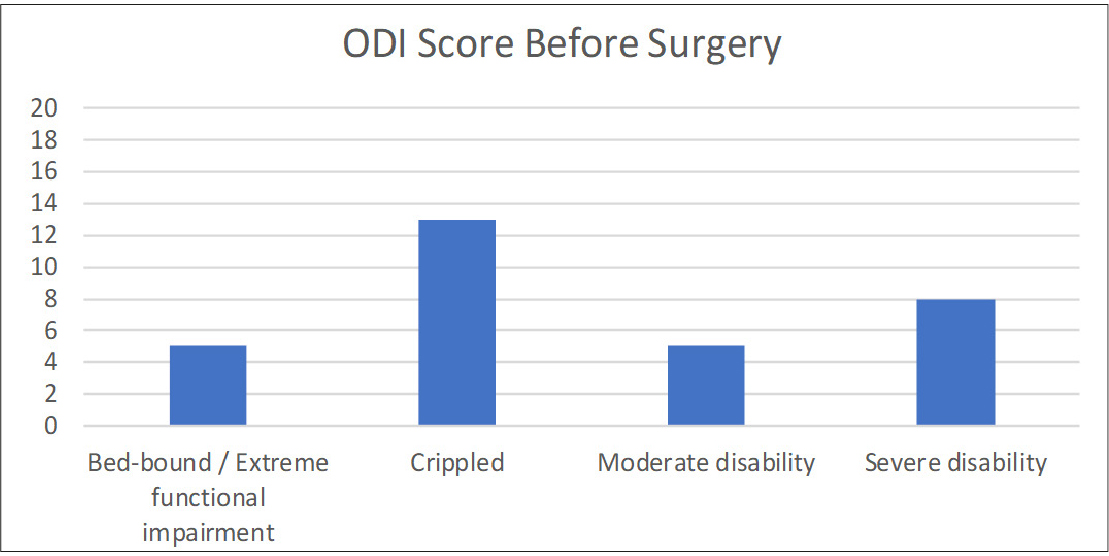
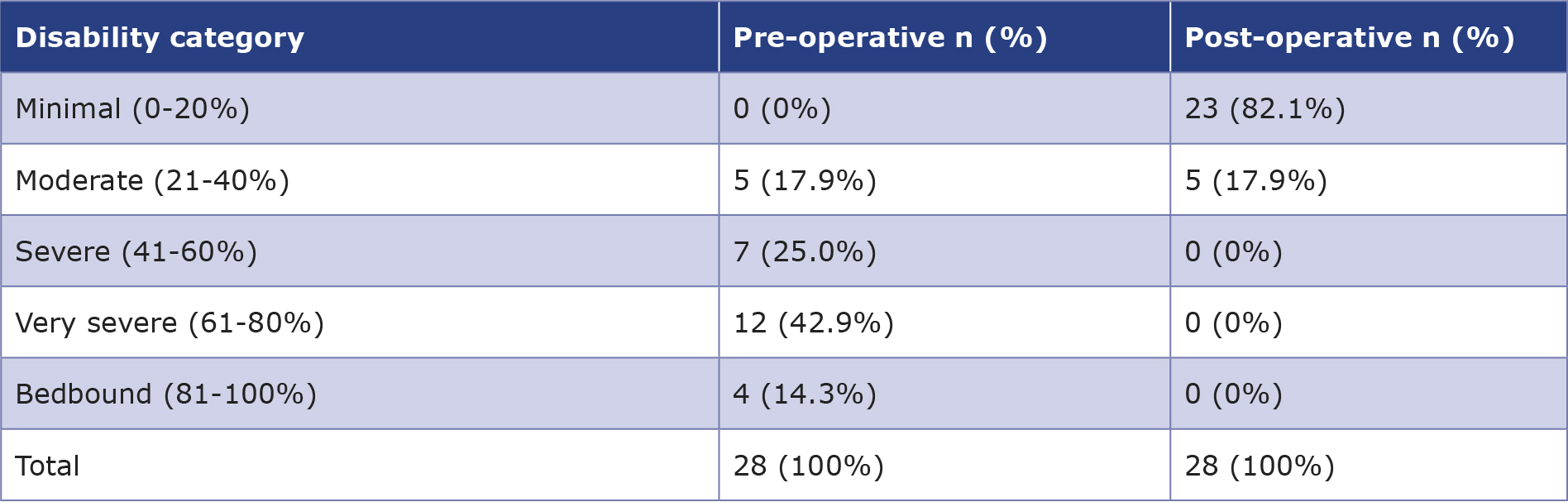
Table 1 presents the ODI scores before and after ELD. The mean change in the ODI score from baseline to post-operative assessment was 50.0 percentage points (95% CI: 44.3- -55.7). A paired t-test demonstrated that this change was statistically significant: t(27) = 27.3, p < 0.0001, representing a large effect size (Cohen’s d = 5.14). Table 2 presents the distribution of patients across ODI disability categories before and after surgery (see Figures 2.1 and 2.2). This represents a clinically and statistically significant shift toward lower disability categories, with 82.1% of patients achieving minimal disability status post-operatively compared to 0% pre-operatively.
Table 1. Summary of Oswestry Disability Index (ODI) scores before and after endoscopic lumbar decompression (n = 28)
Table 2. Distribution of patients by ODI disability category before and after endoscopic lumbar decompression (n = 28)
Figure 2.1. Preoperative Oswestry Disability Index (ODI) scores recorded before ELD (n = 28)
Figure 2.2. ODI Score after ELD
Primary outcome: pain (Numerical Rating Scale)
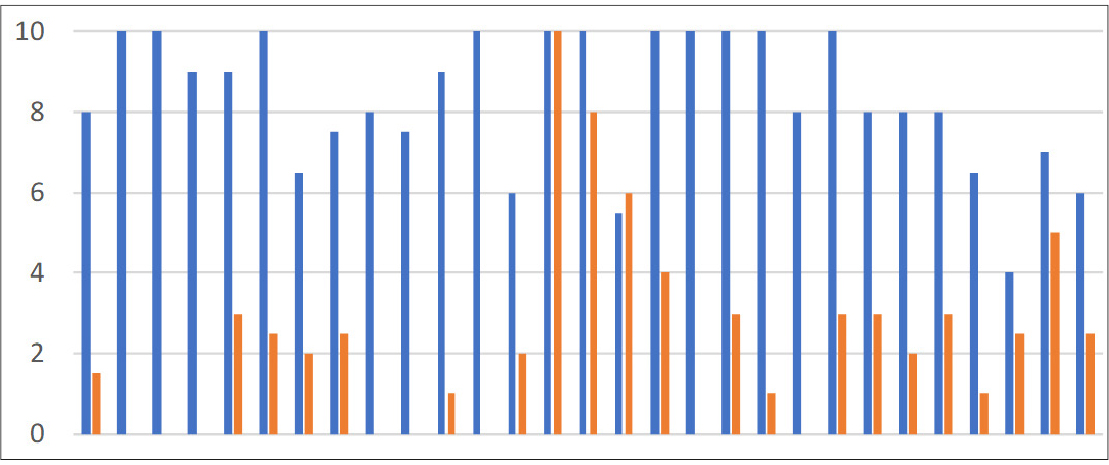
The mean reduction in pain was 5.97 points on the NRS scale (95% CI: 5.09-6.85). A paired t-test demonstrated statistical significance: t(27) = 19.2, p < 0.0001, representing a large effect size (Cohen’s d = 3.64). In the current cohort, 26 of 28 patients (92.9%) met the MCID threshold of ≥ 2.0 points, indicating substantial clinically meaningful improvement in pain (Table 3 and Figure 3).
Table 3. Summary of Numerical Rating Scale (NRS) pain scores before and after endoscopic lumbar decompression (n = 28)
Figure 3. Chart comparing patient self-assessment of pain on the numerical rating scale (NRS) before and after (ELD) (n = 28)
blue bars – NRS assessment before ELD, orange bars – NRS assessment after ELD
Secondary outcomes: functional recovery and satisfaction
Of the 28 patients, 24 (85.7%) reported return to their baseline occupation or equivalent employment duties by final follow-up assessment. Twenty-six of 28 patients (92.9%) reported the successful resumption of activities of daily living(including household activities, self-care, and personal hygiene) without significant functional limitations at final follow-up.
Patient satisfaction, assessed via a Likert scale, was highly favorable: 26 of 28 patients (92.9%) reported being satisfied or very satisfied with the procedure, 2 of 28 patients (7.1%) reported neutral satisfaction, and zero patients (0%) reported dissatisfaction.
Discussion
In this retrospective study we observed significant improvements in both functional disability and pain outcomes of 28 patients, who underwent single-port ELD during the early adoption phase of this procedure at our institution. Mean ODI scores decreased by 50.0 percentage points (from 65.1% to 15.1%, p < 0.0001), with 82.1% of patients transitioning from severe or very severe disability categories to minimal disability post-operatively. Similarly, mean NRS pain scores decreased by 5.97 points (from 8.33 to 2.36, p < 0.0001), with 92.9% of patients achieving the MCID threshold. These results demonstrate that even when performed by surgeons in the early stages of their learning curve, the ELD procedure can produce clinically meaningful improvements in patient-reported outcomes.
Our findings are consistent with those reported by Leyendecker et al., who demonstrated significant early improvements in both ODI and NRS scores after full endoscopic spine surgery in a larger cohort [7]. The magnitude of improvement observed in our study (Cohen’s d = 5.14 for ODI and 3.64 for NRS) indicates large effect sizes, suggesting that the clinical benefits of ELD are substantial and not merely statistically significant. The high rate of return to work (85.7%) and patient satisfaction (92.9%) further supports the clinical effectiveness of this approach.
However, equally notable are the 10.7% intraoperative conversion rate and the 10.7% complication rate (2 instances of post-operative paresis and 1 recurrence) in our series. Both rates are higher than those reported in large- -volume centers with experienced endoscopic surgeons and likely reflect the early learning curve of our surgical team [5-6]. Sun et al. havepreviously documented that complication rates decrease as surgeons progress along the learning curve for percutaneous endoscopic lumbar discectomy [8]. Similarly, Kang et al. found that outcomes of endoscopic surgery improve significantly with increasing surgeon experience [4]. Our surgeons reported subjective improvement in their endoscopic skills during the study period, however, we lacked specific analytical data, such as changes in operating time, to objectively quantify this progression.
The long-term recurrence rate of disc-related pathology following endoscopic procedures remains an important area of ongoing investigation. Several studies have reported recurrence rates ranging from 3% to 12% [15-17], but extended follow-up data beyond 5 years remain limited [18].
Study limitations
Our study has several limitations that should be acknowledged when interpreting the results. The small sample size (n = 28) limits the generalizability of our findings to larger patient populations. Although the data shows promising improvements in both pain and disability, larger cohorts are needed to confirm these findings with more robust statistical power.
We tracked outcomes during a short post-operative period (mean 4.5 months), and therefore we did not collect longterm follow-up data (e.g. recurrence) of disc-related issues or lasting functional improvements. We assessed cases from a single center, focusing on the experiences of a particularsurgical team. Therefore, our findings may not apply to other settings with different levels of ELD expertise or resources.
Patient-reported outcome measures (e.g. the ODI and NRS) may demonstrate only subjective improvements. We were unable to assess objective functional tests or radiological images systematically, which could have enhanced the thoroughness and relevance of the results.
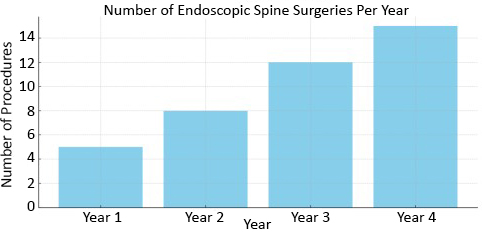
The early stage of adopting ELD at our center involved a significant learning curve (Figure 4). Operator experience and skill levels during this initial period could have influenced the surgical results (e.g. differences in surgery duration, complication rates) and patient outcomes. We lacked specific data to quantify the surgeons’ actual improvement on this procedure’s learning curve (e.g. decrease in operating time over the years), therefore, our findings regarding learning curve progression were based solely on the surgeons’ self-reported opinions.
Figure 4. The increasing number of endoscopic spine surgeries performed by our team
This upward trend reflects the learning curve associated with the adoption of the technique, as well as the growing experience and confidence of the surgical team in performing these procedures.
To confirm these preliminary findings and to better understand the full scope and limits of ELD, multicenter studies with larger cohorts, standardized methods, and extended follow-up are needed.
Conclusions
Single-port ELD yielded substantial and statistically significant improvements in both functional outcomes and pain relief in this cohort of 28 patients, as demonstrated by a 50.0 percentage-point mean reduction in ODI scores and a 5.97-point mean reduction in NRS pain scores, with 92.9% of patients achieving the MCID threshold. However, the moderate complication rate (10.7%) and intraoperative conversion rate (10.7%) reflect the challenges associated with the early stages of the technical learning curve. Extended follow-up with larger, multicenter cohorts is required to assess longterm recurrence rates, durability of clinical outcomes, and the trajectory of the learning curve for this procedure.
Funding
None.
Conflicts of interest
None to report.
References
| 1. |
Kambin P, Gellman H. Percutaneous Lateral Discectomy of the Lumbar Spine A Preliminary Report. Clin Orthop Relat Res [Internet]. 1983;174:127–32. Available from: https://journals.lww.com/corr/fulltext/1983/04000/percutaneous_lateral_discectomy_of_the_lumbar.17.aspx.
|
| 2. |
Mayer HM, Brock M. Percutaneous endoscopic discectomy: surgical technique and preliminary results compared to microsurgical discectomy. J Neurosurg [Internet]. 1993;78(2):216–25. Available from: https://thejns.org/view/journals/j-neurosurg/78/2/article-p216.xml.
|
| 3. |
Kim M, Kim H-S, Oh SW, Adsul NM, Singh R, Kashlan ON, et al. Evolution of Spinal Endoscopic Surgery. Neurospine [Internet]. 2019;16(1):6–14. Available from: https://e-neurospine.org/journal/view.php?doi=10.14245/ns.1836322.161.
|
| 4. |
Kang K-B, Shin Y-S, Seo E-M. Endoscopic Spinal Surgery (BESS and UESS) Versus Microscopic Surgery in Lumbar Spinal Stenosis: Systematic Review and Meta-Analysis. Glob Spine J [Internet]. 2022;12(8):1943–55. Available from: https://journals.sagepub.com/doi/10.1177/21925682221083271.
|
| 5. |
Yang X, Wu Z. Comparison of postoperative outcomes between endoscopic and traditional lumbar spine surgery. Spine J. 2018;18(4):684–690. Available from: https://doi.org/10.1016/j.spinee.2017.08.260.
|
| 6. |
Ruetten S, Komp M, Merk H, Godolias G. Full-Endoscopic Interlaminar and Transforaminal Lumbar Discectomy Versus Conventional Microsurgical Technique. Spine (Phila Pa 1976) [Internet]. 2008;33(9):931–9. Available from: http://journals.lww.com/00007632-200804200-00002.
|
| 7. |
Leyendecker J, Prasse T, Park C, Payne C, Rückels P, Bieler E, et al. Pain alleviation and functional improvement: ultra-early patient-reported outcome measures after full endoscopic spine surgery. J Neurosurg Spine [Internet]. 2024;40(4):465–74. Available from: https://thejns.org/view/journals/j-neurosurg-spine/40/4/article-p465.xml.
|
| 8. |
Sun B, Shi C, Xu Z, Wu H, Zhang Y, Chen Y, et al. Learning Curve for Percutaneous Endoscopic Lumbar Diskectomy in Bi-needle Technique Using Cumulative Summation Test for Learning Curve. World Neurosurg [Internet]. 2019;129:e586–93. Available from: https://www.sciencedirect.com/science/article/pii/S1878875019315049.
|
| 9. |
Chung AS, Wang JC. The Rationale for Endoscopic Spinal Surgery. Neurospine [Internet]. 2020;17(Suppl 1):S9–12. Available from: http://e-neurospine.org/journal/view.php?doi=10.14245/ns.2040104.052.
|
| 10. |
Kim H-S, Wu PH, Jang I-T. Commentary on “Complications and Management of Endoscopic Spinal Surgery”. Neurospine [Internet]. 2023;20(1):78–9. Available from: http://e-neurospine.org/journal/view.php?doi=10.14245/ns.2346308.154.
|
| 11. |
Fairbank JCT, Pynsent PB. The Oswestry disability index. Spine (Phila Pa 1976) [Internet]. 2000;25(22):2940–53. Available from: https://journals.lww.com/spinejournal/_layouts/15/oaks.journals/downloadpdf.aspx?an=00007632-200011150-00017.
|
| 12. |
Hjermstad MJ, Fayers PM, Haugen DF, Caraceni A, Hanks GW, Loge JH, et al. Studies Comparing Numerical Rating Scales, Verbal Rating Scales, and Visual Analogue Scales for Assessment of Pain Intensity in Adults: A Systematic Literature Review. J Pain Symptom Manage [Internet]. 2011;41(6):1073–93. Available from: https://www.sciencedirect.com/science/article/pii/S0885392411000145.
|
| 13. |
Copay AG, Glassman SD, Subach BR, Berven S, Schuler TC, Carreon LY. Minimum clinically important difference in lumbar spine surgery patients: a choice of methods using the Oswestry Disability Index, Medical Outcomes Study questionnaire Short Form 36, and Pain Scales. Spine J [Internet]. 2008;8(6):968–74. Available from: https://www.sciencedirect.com/science/article/pii/S1529943007010017.
|
| 14. |
Likert R. A technique for the measurement of attitudes. Arch Psychol [Internet]. 1932 [cited 2018 Nov 22];22(140):55. Available from: http://psycnet.apa.org/record/1933-01885-001.
|
| 15. |
Yin S, Du H, Yang W, Duan C, Feng C, Tao H. Prevalence of recurrent herniation following percutaneous endoscopic lumbar discectomy: a meta-analysis. Pain Physician [Internet]. 2018;21(4):337. Available from: https://www.painphysicianjournal.com/current/pdf?article=NTMwMw%3D%3D&journal=112.
|
| 16. |
Park CH, Park ES, Lee SH, Lee KK, Kwon YK, Kang MS, et al. Risk factors for early recurrence after transforaminal endoscopic lumbar disc decompression. Pain Physician [Internet]. 2019;22(2):E133. Available from: https://www.painphysicianjournal.com/current/pdf?article=NjIxNw%3D%3D&journal=119.
|
| 17. |
Tang T, Liu J, Cao J, He D, Cheng X, Xie S. Risk Factors and Causes of Reoperation in Lumbar Disc Herniation Patients after Percutaneous Endoscopic Lumbar Discectomy: A Retrospective Case Series with a Minimum 2-Year Follow-Up. Med Sci Monit [Internet]. 2023;29:e939844. Available from: http://www.ncbi.nlm.nih.gov/pubmed/37580900.
|
| 18. |
Yang X, Zhang S, Su J, Guo S, Ibrahim Y, Zhang K, et al. Comparison of Clinical and Radiographic Outcomes Between Transforaminal Endoscopic Lumbar Discectomy and Microdiscectomy: A Follow-up Exceeding 5 Years. Neurospine [Internet]. 2024;21(1):303–13. Available from: http://www.ncbi.nlm.nih.gov/pubmed/38317550.
|
