


Influence of whey protein and creatine supplementation on liver and kidney function


Abstract
Background: Due to their availability and purported benefits for muscle growth and athletic performance, the use of whey protein and creatine supplements is widespread among recreational and amateur athletes.
Material and methods: 600 gym-goers (24-52 years of age) were divided into 3 groups based on their dietary supplement use: none (group A), moderate amounts (group B) and high doses (group C). Biochemical analysis of kidney and liver function was performed.
Results: High-dose supplementation significantly increased serum creatinine, serum urea and liver enzymes (AST, ALT) and bilirubin levels compared with the control and medium-dose groups. Group C showed the highest creatinine (1.33 ± 0.216 mg/dL) and serum urea (55.31 ± 6.49 mg/dL), suggesting a possible association with renal function biomarkers. Similarly, AST and ALT levels were significantly increased in supplement users (particularly in group C), suggesting increased transient variations in hepatic enzyme activity.
Conclusions: Our findings highlight a dose-dependent effect of whey protein and creatine supplementation on liver and kidney function, and emphasize the importance of responsible dietary supplement use and periodic monitoring of biochemical markers.
Citation
Barani S, Mahmood A, Kamal I. Influence of whey protein and creatine supplementation on liver and kidney function. Eur J Transl Clin Med. 2026;9(1):66-72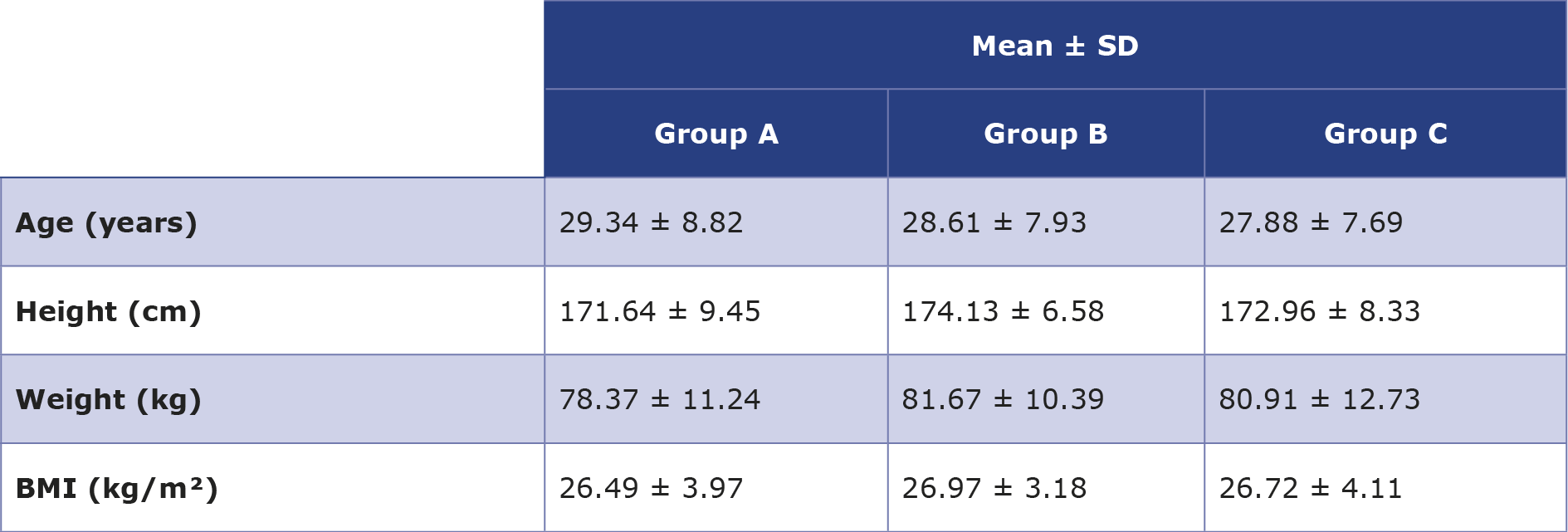





Introduction
Whey protein (WP) in particular, a component of milk protein, has become popular for muscle building and weight management [1]. Despite the growing interest in nutritional supplementation among physically active people, data on the use of exercise supplements are limited [2]. It is estimated that 32-90% of athletes use dietary supplements [3].
Proteins such as β-lactoglobulin, α-lactalbumin, immunoglobulins and bovine serum albumin, which are obtained from the liquid by-product of milk following cheese production through enzymatic coagulation and subsequent purification processes [4]. These include many of the well-known branched-chain amino acids of WP. Studies show that WP is the most popular protein supplement among athletes, contributing to protein synthesis, increased lean muscle mass, and carbohydrate metabolism [5].
Many physically active people use WP without medical guidance and few studies examine the safety and adverse effects of such supplements. Excessive WP intake can lead to periodontal disease, diarrhea, microbial dysfunction and changes in kidney and liver metabolism [6]. It is necessary to differentiate the outcomes derived from animal studies from those observed in patients with pre-existing illnesses and in healthy people. Most reported adverse renal or hepatic effects from high protein or creatine intake come from animal studies or patients already having existing illnesses related to the kidneys or the liver, while there are inconsistent data from healthy recreational athletes or active individuals among whom no significant changes were observed [7-8].
Post-exercise protein intake is necessary to increase and balance muscle protein synthesis, supporting hypertrophy. Taking 40 g of casein before sleep improves nocturnal protein synthesis and recovery compared to carbohydrates, this process can increase muscle strength and growth over time [9]. High dietary protein intake can lead to kidney problems, e.g. hyperfiltration, glomerular injury, and proteinuria, which can lead to chronic kidney disease (CKD) Animal protein diet is the highest risk factor end-stage kidney disease (ESKD) is associated due to factors such as acid load and inflammation It should be the former, especially for those at risk [10].
Although though high protein intake has been associated with elevated glomerular filtration rate and a greater workload of the kidney, there is current evidence indicating this does not necessarily result in kidney injury among healthy individuals. This could be the case among those who already have kidney problems, though [11].
Creatine, a compound composed of the amino acids arginine methionine and glycine, is produced through diet and metabolism. Creatine supplements are a promising ergogenic adjuvant that enhance athletic performance during short-term intense exercise and are widely used by both professional athletes and the general public [12]. Consistent reports show that creatine supplementation increases muscle creatine and phosphocreatine levels [13]. This increases the availability of phosphocreatine, increases the cellular efficiency of the phosphogenic system and facilitates the transport of high-energy phosphate between the cytosol and the mitochondria through creatine phosphate interactions [14].
In some cases, people need to get enough creatine from their diet to meet a certain level of nutritional needs [15]. Dietary creatine is generally considered safe, although excessive levels can cause gastrointestinal discomfort. Some preclinical studies and data suggest that exogenous creatine may adversely affect liver function by increasing liver enzymes, exacerbating ethanol-induced alteration in liver enzyme markers, and potentially leading to changes in hepatic biomedical parameters [16]. However, the effect of dietary creatine on biomarkers of liver health in the general population remains unclear. The indiscriminate use of creatine supplements has raised safety concerns, particularly with respect to possible changes in the liver and kidneys [17].
Although WP or creatine supplementation at recommended dosages does not cause significant changes in the liver or kidney function of healthy subjects, there are evolving data implicating high doses of these supplements in detectable changes in serum creatinine, urea, and liver enzyme levels [18]. Accordingly, the purpose of our study was to assess the influence of WP and creatine supplementation on the chosen liver and kidney function parameters in healthy participants, especially focusing on the differences between physiological and clinically significant values.
Material and methods
This cross-sectional analytical study was carried out in Ninawa (Iraq), from September 2023 to April 2024. The participants regularly trained at gyms in different locations within the city. They were interviewed to respond to the questionnaires directly, supplement intake was assessed using a self-reported questionnaire. The questions focused on the quantity of taking supplement and other types of food taken daily. Information regarding diet was collected using a 24-hour recall procedure conducted on 3 non-consecutive days, consisting of 2 weekdays and 1 weekend day. Total daily protein intake was calculated by adding protein obtained from diet and protein supplements.
This was followed by biochemical tests to investigate the liver and kidney function. Ethical approval for this study was obtained from the Collegiate Committee for Medical Research Ethics at the University of Mosul. Informed consent was obtained from the participants.
Participants
All participants (600) in this study were male, 24 to 52 years of age who regularly trained at the gym 6 days/week, averaging 1 hour per day. Resistance training comprised the major part of their exercise. To avoid confounding by training, gym-goers who reported changes in training intensity, volume or type during the preceding month were not recruited. The rest of the exclusion criteria were as follows: females, coaches, professional athletes, hormone supplement use, chronic health conditions (e.g. diabetes, liver and kidney disease). The participants were divided into 3 equal groups. Group A included participants who did not consume WP and creatine supplements. Those in group B taking 30 grams (g) of WP and 5 g creatine, and group C taking 45 g of WP and 7.5 g creatine. The participants in groups B and C were requested to use WP and creatine supplements at least 8 weeks before blood sample collection. This ensured that the supplementation usage period was sufficient enough to allow any biochemical changes to occur.
Biochemical analysis
Consumption of total protein was determined using 24 hours recall combined with a meal replacement list. Body mass index (BMI) was calculated using the standard formula (weight (kg)/height (m²)). A total of 5 ml of venous blood was collected, left to clot and centrifuged to obtain serum for biochemical analysis of liver function tests (AST, ALT, total bilirubin and direct bilirubin and kidney function tests (serum creatinine and urea). All participants were instructed to maintain their usual hydration status and to avoid vigorous exercise and alcohol consumption 24 hours prior to blood sampling.
Statistical analysis
The study data were analyzed using the SPSS software (version 24, IBM Corp., Armonk, USA). Normality for continuous variables was determined using the Shapiro-Wilk test. The homogeneity of variance assumption was checked by Levene’s test. Variables within groups were compared using the chi-square test. Continuous variable of liver and kidney function served as depended variables and were compared by t-test. In situations requiring comparison of more than two groups, one-way ANOVA, combined with post hoc Tukey’s test, was used to account for multiple comparison issues. Differences were considered statistically significant at p < 0.05. For continuous variables, the effect size in terms of Cohen’s d was determined together with the 95% confidence interval.
Results
Age, weight, height and BMI of all participants are shown in Table 1 and no statistically significant differences between them were observed.
Table 1. Comparisons of mean age, height, weight and BMI among the 3 groups of participants
Kidney function
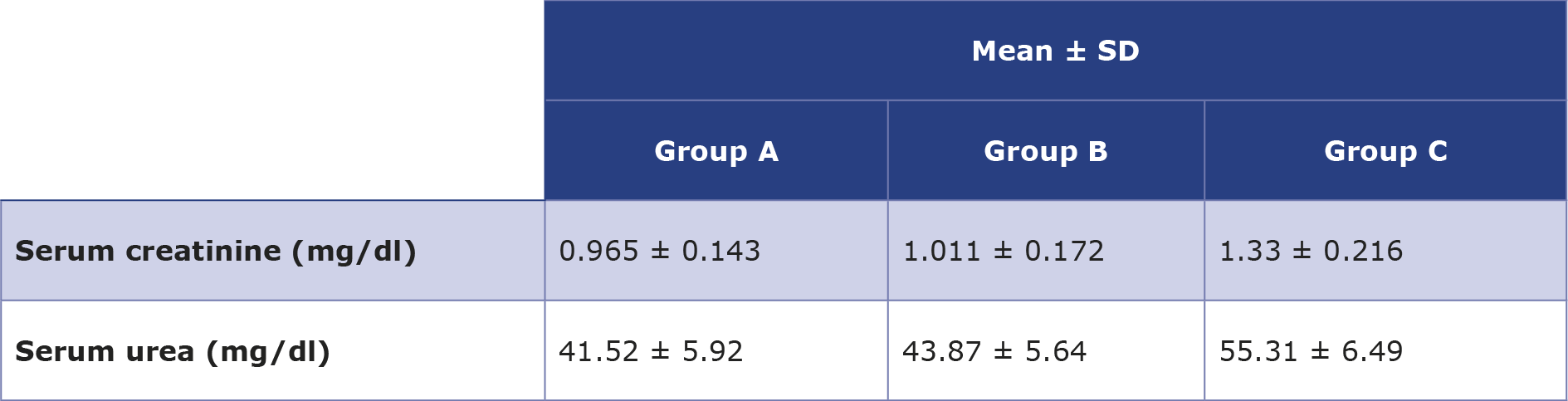
Our results demonstrated that the mean level of serum creatinine in the A, B and C groups were 0.965 ± 0.143 mg/dL, 1.011 ± 0.172 mg/Dl and 1.33 ± 0.216 mg/dL, respectively. This reveals that the participants in group A (who did not consume WP and creatine supplements) had normal serum creatinine. However, group B showed a significant increase in serum creatinine compared with group A. In addition, comparing with group A and B, those in group C had significantly higher levels of serum creatinine (Table 2). Such high serum creatinine levels may in part represent an association with muscle mass or creatine-produced creatinine, which are common in physically active people and not indicative of renal biomarker changes [7].
Table 2. Renal function parameters in the 3 groups of participants
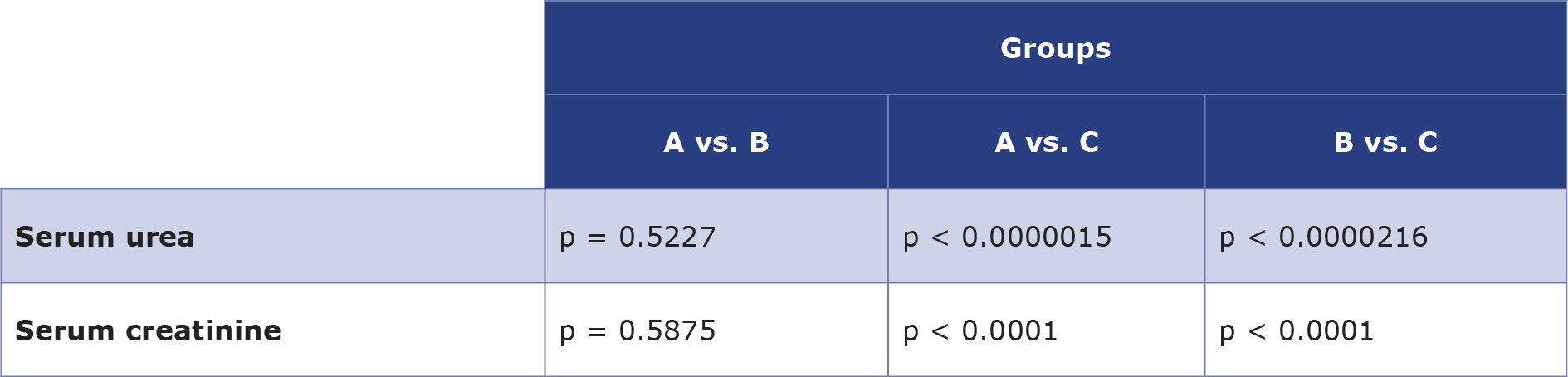
In addition, the mean level of serum urea in A, B and C groups were 41.52 ± 5.92 mg/dL, 43.87 ± 5.64 mg/dL and 55.31 ± 6.49 mg/dL, respectively. There was only a significant increase in serum urea in group C in comparison with both group A and B as shown in Table 3. Although there were significant differences in the levels of serum creatinine and urea, their results have been cautiously interpreted in the context of exercise, muscle mass and creatine supplements.
Table 3. The p value for each pair ways tow sample t-test for each of the parameters (serum urea and serum creatinine)
Liver function tests
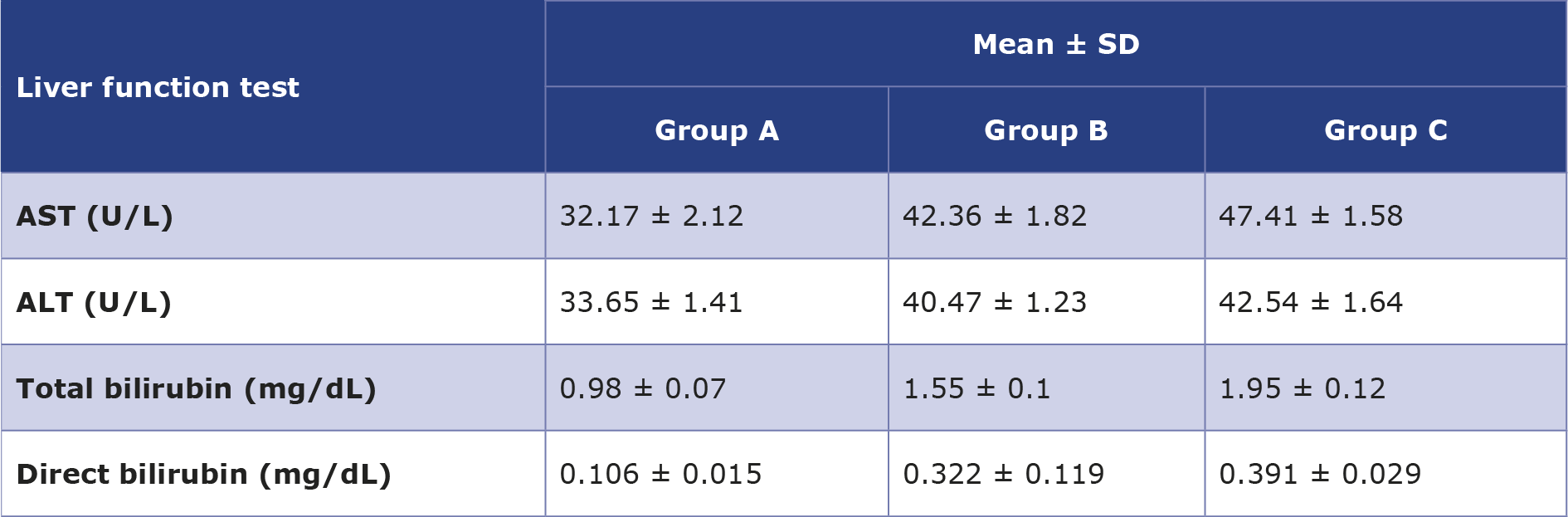
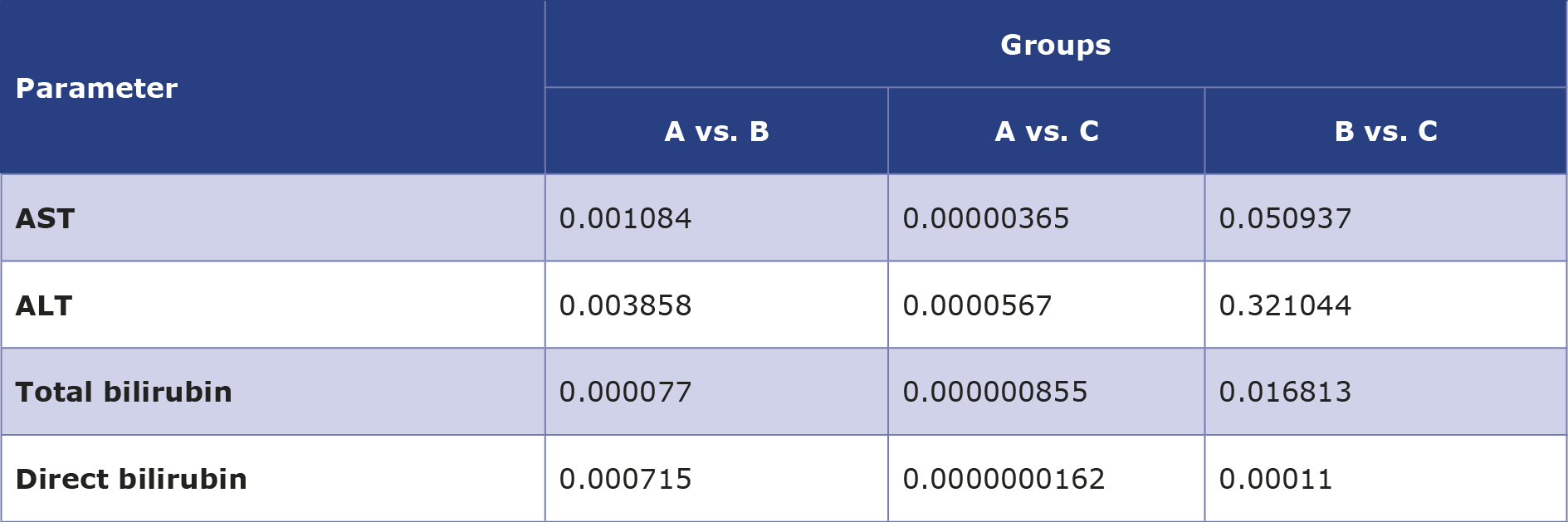
The mean level of serum AST in groups B and C was higher (42.36 ± 1.82 U/L and 47.41 ± 1.58 U/L, respectively) than in group A (32.17 ± 2.12 U/L) (Table 4). In addition, the mean level of serum ALT was also elevated in groups B and C were (40.47 ± 1.23 U/L and 42.54 ± 1.64 U/L, respectively), compared to group A (33.65 ± 1.41 U/L). Groups B and C had significantly higher ALT than the group A, whilst no significant difference was found between groups B and C (Table 4). Furthermore, the mean levels of total bilirubin in groups A, B and C were 0.98 ± 0.07 mg/dL, 1.55 ± 0.1 mg/dL, 1.95 ± 0.12 mg/dL, respectively. The differences in total bilirubin between groups B and A as well as C and A were statistically significant. In addition, significant difference was also noted between groups B and C, as shown in the Table 5.
Table 4. Liver function parameters in the 3 groups of participants
Table 5. The p value for each paired two sample t-test for each of the parameters (AST, ALT, total bilirubin and direct bilirubin)
Discussion
Our findings provide an insight into the effects of WP and creatine supplements on kidney and liver function in gym-goers. Although the consumption of WP and creatine and their effect on kidney and liver function are still controversial, same reports found that WP protects against hypertension and a wide range of metabolic disease (e.g. dyslipidemia, type 2 diabetes and obesity) [6]. Similarly to other studies, our data suggests that low dose supplementation of WP and creatine has no effect on the kidney and liver function [19].
The significantly increased levels in group C suggest that high-dose supplementation may increase creatinine production and retention, potentially due to increased muscle metabolism or decreased renal clearance. Higher creatinine level may also represent a higher muscle mass or creatinine production from creatine supplements and not necessarily renal functional biomarkers changes, particularly in people with high activity physical levels [7]. Elevated creatinine levels were associated with increased renal biomarkers due to high protein intake, which is consistent with findings in previous research demonstrating the potential effect of excessive WP supplementation on kidney function [20-21].
In addition, serum urea levels had a similar pattern in the groups. While there were no significant differences between groups A and B, group C showed significantly higher levels, indicating altered kidney function probably due to increased nitrogenous waste from higher protein metabolism, as confirmed by earlier studies. Urea (or blood urea nitrogen, BUN) is a nitrogen-containing substance produced in the liver during the urea cycle as a byproduct of protein metabolism. Around 85% of urea removed by the kidneys, while the remainder is excreted through the gastrointestinal system [20-22].
Elevations of liver enzymes (AST) and ALT levels were observed in groups B and C. These results suggest that WP and creatine use are associated with increased liver enzyme activity, indicating transient variations in liver biochemical markers. Previous reports associate WP intake with minor changes in liver enzymes, particularly in individuals with underlying disease or who excessively consume WP [1]. In addition, both total and direct bilirubin levels were significantly increased in groups B and C compared with group A, suggesting a dose- -dependent effect of supplementation on bilirubin metabolism. Our findings are consistent with previous studies that caution against unsupervised supplement use due to possible disruption of liver detoxification pathways [22-23].
The liver plays a central role in protein metabolism, particularly in the deamination and transamination processes that break down amino acids. Supplementation with WP and creatine results in increased availability of amino acids in the bloodstream, requiring the liver to metabolize these excess substrates. This increased metabolic activity may increase the expression and release of liver enzymes such as AST and ALT into the bloodstream, as they are markers of hepatocyte activity or damage [24]. Furthermore, the elevation of transaminases secondary to exercise and/or WP and creatine supplementation also demands consideration, as these are not always indicative of hepatocellular damage in physically active populations [25]. Creatine, if consumed in excess, undergoes metabolism to form creatinine, primarily in the liver. This additional metabolic burden could lead to mild stress on the hepatocytes, causing enzymes to be released into the circulation. Studies have shown that prolonged or excessive creatine supplementation is associated with mild but reversible increases in liver enzyme levels [26].
Limitations of this study
Our study has several limitations. First and foremost, this was a the cross-sectional analysis without long-term data. Supplement intake was self-reported in our study. Furthermore, serum creatinine may not be a precise indicator of kidney function in physically active people. Unfortunately, we did not measure the participants’ eGFR and other renal biomarkers. Finally, we did not analyze the possible role of dietary and exercise-related covariates. Therefore, our results cannot and should not be generalized to all physically active individuals.
Conclusions
This study demonstrated that high-dose WP and creatine supplementation is associated with elevations in several biochemical markers of liver and kidney function. Moderate supplementation, however, did not produce significant changes. Although these findings suggest potential physiological effects, they do not necessarily indicate organ damage or clinical dysfunction. Our results underscore the value of overseeing supplement intake by coach or dietician and interpreting changes in biochemical markers within the context of exercise, muscle mass, and creatine metabolism. Further longitudinal studies measuring additional renal and liver biomarkers are recommended to clarify the clinical relevance of these associations.
Acknowledgments
The authors would like to express their gratitude to the College of Pharmacy at the University of Mosul, for providing the support and facilities required to conduct this study. We extend our heartfelt appreciation to all laboratory Staff, whose support contributed to the completion of this study.
Funding
None.
Conflicts of interest
None to report.
----
Image source: pexels.com
References
| 1. |
Cava E, Padua E, Campaci D, Bernardi M, Muthanna FMS, Caprio M, et al. Investigating the Health Implications of Whey Protein Consumption: A Narrative Review of Risks, Adverse Effects, and Associated Health Issues. Healthcare [Internet]. 2024;12(2):246. Available from: https://www.mdpi.com/2227-9032/12/2/246.
|
| 2. |
Ruano J, Teixeira VH. Prevalence of dietary supplement use by gym members in Portugal and associated factors. J Int Soc Sports Nutr [Internet]. 2020;17(1). Available from: https://www.tandfonline.com/doi/full/10.1186/s12970-020-00342-z.
|
| 3. |
Giannopoulou I, Noutsos K, Apostolidis N, Bayios I, Nassis GP. Performance level affects the dietary supplement intake of both individual and team sports athletes. J Sports Sci Med [Internet]. 2013;12(1):190–6. Available from: http://www.ncbi.nlm.nih.gov/pubmed/24149744.
|
| 4. |
Minj S, Anand S. Whey Proteins and Its Derivatives: Bioactivity, Functionality, and Current Applications. Dairy [Internet]. 2020;1(3):233–58. Available from: https://www.mdpi.com/2624-862X/1/3/16.
|
| 5. |
Pasiakos SM, McLellan TM, Lieberman HR. The Effects of Protein Supplements on Muscle Mass, Strength, and Aerobic and Anaerobic Power in Healthy Adults: A Systematic Review. Sport Med [Internet]. 2015;45(1):111–31. Available from: http://link.springer.com/10.1007/s40279-014-0242-2.
|
| 6. |
Vasconcelos QDJS, Bachur TPR, Aragão GF. Whey protein supplementation and its potentially adverse effects on health: a systematic review. Appl Physiol Nutr Metab [Internet]. 2021;46(1):27–33. Available from: https://cdnsciencepub.com/doi/10.1139/apnm-2020-0370.
|
| 7. |
Kreider RB, Kalman DS, Antonio J, Ziegenfuss TN, Wildman R, Collins R, et al. International Society of Sports Nutrition position stand: safety and efficacy of creatine supplementation in exercise, sport, and medicine. J Int Soc Sports Nutr [Internet]. 2017;14(1). Available from: https://www.tandfonline.com/doi/full/10.1186/s12970-017-0173-z.
|
| 8. |
Poortmans JR, Dellalieux O. Do Regular High Protein Diets Have Potential Health Risks on Kidney Function in Athletes? Int J Sport Nutr Exerc Metab [Internet]. 2000;10(1):28–38. Available from: https://journals.humankinetics.com/view/journals/ijsnem/10/1/article-p28.xml.
|
| 9. |
West D, Abou Sawan S, Mazzulla M, Williamson E, Moore D. Whey Protein Supplementation Enhances Whole Body Protein Metabolism and Performance Recovery after Resistance Exercise: A Double-Blind Crossover Study. Nutrients [Internet]. 2017;9(7):735. Available from: https://www.mdpi.com/2072-6643/9/7/735.
|
| 10. |
Ko G-J, Rhee CM, Kalantar-Zadeh K, Joshi S. The Effects of High-Protein Diets on Kidney Health and Longevity. J Am Soc Nephrol [Internet]. 2020;31(8):1667–79. Available from: https://journals.lww.com/10.1681/ASN.2020010028.
|
| 11. |
Martin WF, Armstrong LE, Rodriguez NR. Dietary protein intake and renal function. Nutr Metab (Lond) [Internet]. 2005;2(1):25. Available from: https://nutritionandmetabolism.biomedcentral.com/articles/10.1186/1743-7075-2-25.
|
| 12. |
de Souza e Silva A, Pertille A, Reis Barbosa CG, Aparecida de Oliveira Silva J, de Jesus DV, Ribeiro AGSV, et al. Effects of Creatine Supplementation on Renal Function: A Systematic Review and Meta-Analysis. J Ren Nutr [Internet]. 2019;29(6):480–9. Available from: https://www.sciencedirect.com/science/article/pii/S1051227619302286.
|
| 13. |
Heaton LE, Davis JK, Rawson ES, Nuccio RP, Witard OC, Stein KW, et al. Selected In-Season Nutritional Strategies to Enhance Recovery for Team Sport Athletes: A Practical Overview. Sport Med [Internet]. 2017;47(11):2201–18. Available from: https://doi.org/10.1007/s40279-017-0759-2.
|
| 14. |
Wallimann T, Dolder M, Schlattner U, Eder M, Hornemann T, O’Gorman E, et al. Some new aspects of creatine kinase (CK): compartmentation, structure, function and regulation for cellular and mitochondrial bioenergetics and physiology. BioFactors [Internet]. 1998;8(3–4):229–34. Available from: https://doi.org/10.1002/biof.5520080310.
|
| 15. |
Ostojic SM, Forbes SC. Perspective: Creatine, a Conditionally Essential Nutrient: Building the Case. Adv Nutr [Internet]. 2022;13(1):34–7. Available from: https://www.sciencedirect.com/science/article/pii/S2161831322005269.
|
| 16. |
Marinello PC, Cella PS, Testa MTJ, Guirro PB, Brito WAS, Borges FH, et al. Creatine supplementation exacerbates ethanol-induced hepatic damage in mice. Nutrition [Internet]. 2019;66:122–30. Available from: https://www.sciencedirect.com/science/article/pii/S0899900719300693.
|
| 17. |
Todorovic N, Korovljev D, Stajer V, Jorga J, Ostojic SM. Creatine consumption and liver disease manifestations in individuals aged 12 years and over. Food Sci Nutr [Internet]. 2023;11(2):1134–41. Available from: https://onlinelibrary.wiley.com/doi/10.1002/fsn3.3151.
|
| 18. |
Pline KA, Smith CL. The Effect of Creatine Intake on Renal Function. Ann Pharmacother [Internet]. 2005;39(6):1093–6. Available from: https://journals.sagepub.com/doi/10.1345/aph.1E628.
|
| 19. |
Wirunsawanya K, Upala S, Jaruvongvanich V, Sanguankeo A. Whey Protein Supplementation Improves Body Composition and Cardiovascular Risk Factors in Overweight and Obese Patients: A Systematic Review and Meta-Analysis. J Am Coll Nutr [Internet]. 2018;37(1):60–70. Available from: https://doi.org/10.1080/07315724.2017.1344591.
|
| 20. |
Schlickmann DS, Molz P, Brand C, dos Santos C, da Silva TG, Rieger A, et al. Liver and kidney function markers among gym users: the role of dietary supplement usage. Br J Nutr [Internet]. 2021/09/13. 2022;128(4):704–11. Available from: https://www.cambridge.org/core/product/A5C351DDCDA7C1E5F69FD37D4394B425.
|
| 21. |
Souza RA, Miranda H, Xavier M, Lazo-Osorio RA, Gouvea HA, Cogo JC, et al. Effects of high-dose creatine supplementation on kidney and liver responses in sedentary and exercised rats. J Sports Sci Med [Internet]. 2009;8(4):672–81. Available from: http://www.ncbi.nlm.nih.gov/pubmed/24149610.
|
| 22. |
Tawfik MS, Al-Badr N. Adverse Effects of Monosodium Glutamate on Liver and Kidney Functions in Adult Rats and Potential Protective Effect of Vitamins C and E. Food Nutr Sci [Internet]. 2012;03(05):651–9. Available from: https://www.scirp.org/journal/paperinformation?paperid=19078.
|
| 23. |
D’Lugos A, Luden N, Faller J, Akers J, McKenzie A, Saunders M. Supplemental Protein during Heavy Cycling Training and Recovery Impacts Skeletal Muscle and Heart Rate Responses but Not Performance. Nutrients [Internet]. 2016;8(9):550. Available from: https://www.mdpi.com/2072-6643/8/9/550.
|
| 24. |
Candow DG, Forbes SC, Chilibeck PD, Cornish SM, Antonio J, Kreider RB. Effectiveness of Creatine Supplementation on Aging Muscle and Bone: Focus on Falls Prevention and Inflammation. J Clin Med [Internet]. 2019;8(4):488. Available from: https://www.mdpi.com/2077-0383/8/4/488.
|
| 25. |
Brancaccio P, Lippi G, Maffulli N. Biochemical markers of muscular damage. cclm [Internet]. 2010;48(6):757–67. Available from: https://www.degruyter.com/document/doi/10.1515/CCLM.2010.179/html.
|
| 26. |
Ziegenfuss TN, Rogers M, Lowery L, Mullins N, Mendel R, Antonio J, et al. Effect of creatine loading on anaerobic performance and skeletal muscle volume in NCAA division I athletes. Nutrition [Internet]. 2002;18(5):397–402. Available from: https://www.sciencedirect.com/science/article/pii/S0899900701008024.
|
