

Novel cardiovascular risk factors in young women with classical risk profiles


Abstract
Introduction: Urbanization plays a growing role in the development of atherosclerotic cardiovascular disease (ASCVD) across the Middle East, particularly among younger adults. Yet, we still know very little about how the health profiles of young women differ between urban and rural settings. In this study, we aim to bridge that gap by examining the demographic characteristics and the prevalence of both classical and novel ASCVD risk factors in young Middle Eastern women.
Methods: We analyzed the demographic, social, and clinical profiles of women aged 18-50 years, including 19 classical and novel ASCVD risk factors. We included participants living in either urban or rural areas, recruited from 11 centers across Jordan and 1 in the Gaza Strip between August 2020 and October 2023.
Results: Of the 627 women studied (mean age 44.2 ± 5.1 years), 74% lived in urban areas and 26% in rural areas. ASCVD was present in 32.0% of urban and 37.3% of rural participants. Rural women had higher rates of physical inactivity, obesity, and elevated BMI, while smoking was more common among urban women. Among novel risk factors, premature menopause and depression were more frequent in urban women, whereas hypertensive disorders of pregnancy were more common in rural women.
Conclusion: Urban young women demonstrated a worse clinical profile, with higher prevalence of several key ASCVD risk factors.
Citation
Ibdah A, Alkhawaldeh M, Ibdah R, Hulliel A, Rawashdeh S, Al-Akhras A, Abedal-Kareem K, Wahbeh L, Khader S, Baker M, Eid S, Mansi J A, Khraisat R, Alsahan M H, Al-Rhayyel Y, Alawajneh M M, Dayah S A, Mahmoud S, Hammoudeh A. Novel cardiovascular risk factors in young women with classical risk profiles. Eur J Transl Clin Med.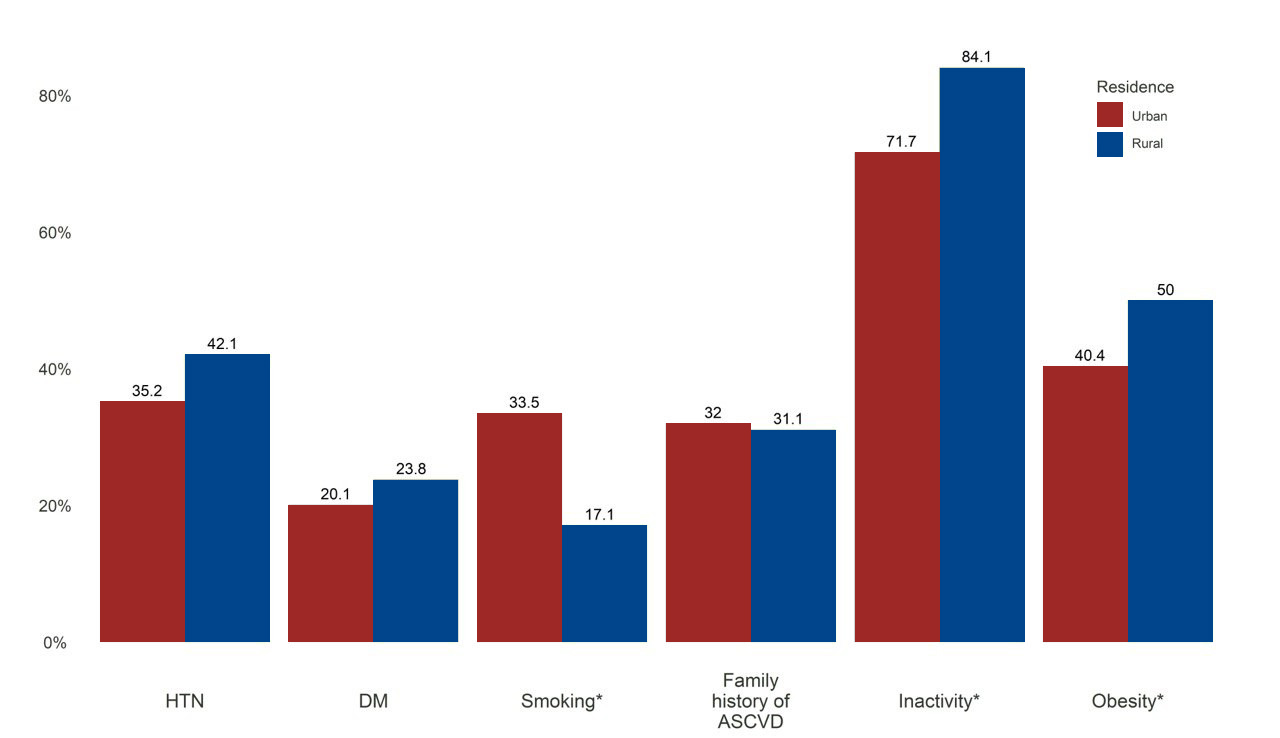



Introduction
Atherosclerotic cardiovascular disease (ASCVD) has become a major global epidemic, accounting for nearly one-- third of all deaths worldwide [1]. In Jordan, ASCVD was responsible for 45% of all deaths in 2019, according to the Ministry of Health [2]. Across the Middle East and North Africa (MENA), the number of ASCVD cases increased by 140.9% between 1990 and 2019 [3]. Although women experience ASCVD at rates similar to men, evidence shows they often suffer higher mortality and worse outcomes after acute cardiovascular (CV) events [4]. The long-held belief that women are protected from ASCVD is false because the data shows that almost half of all women will develop heart disease or experience a stroke during their lifetime [5-6]. Notably, acute myocardial infarction in the Middle East occurs at a younger age compared with other regions [3, 7]. Classical (traditional) ASCVD risk factors (e.g. diabetes mellitus (DM), hypertension (HTN), smoking, dyslipidemia, obesity, family history of premature ASCVD, physical inactivity) vary even within the same country. One in six women with type 2 diabetes (T2DM) in the Middle East and Africa experience early ASCVD, with most at high or very high risk for an acute CV event [8]. HTN is also highly prevalent, and about 10% of untreated individuals develop ASCVD [9-10]. Smoking further increases risk, with women who smoke facing a 25% higher CV risk than men of the same age. Hypercholesterolemia contributes substantially as well, accounting for 47% of the population-adjusted CV risk in women [11]. Family history of premature ASCVD remains another key risk factor, affecting around 2.3% of the population and associated with recurrent events [12]. Emerging evidence has highlighted several female-specific and reproductive age-related novel risk factors (including gestational diabetes mellitus (GDM), hypertensive disorders of pregnancy (HDP), preterm delivery, postpartum weight gain, polycystic ovary syndrome, and premature menopause) that contribute to ASCVD development in young women [13]. Our aim was to bridge this gap by investigating the variations in clinical and socioeconomic characteristics encompassing classical and novel CV risk factors within a cohort of Middle Eastern women.
Material and methods
This study is based on data from the Novel and Classical Atherosclerotic Cardiovascular Risk Factors in Middle Eastern Young Women (ANCORS-YW) Study. The detailed methodology has been described earlier [14]. In summary, this was a case-control, cross-sectional multicenter study conducted between August 2021 and October 2023, and it follows the STROBE guidelines for reporting observational research. Participants were recruited from 12 centers, including 11 across Jordan and one in the Gaza Strip. The sample size was calculated using a significance level of 0.05, a power of 80%, and an estimated frequency of 10% for each variable. Based on these assumptions, and to detect a clinically meaningful difference between the study groups (odds ratio = 2%), the required total sample size was 627 participants (209 cases and 418 controls).
Cases included married women aged 18-50 years who had ASCVD and at least 1 previous pregnancy. Each case was matched by age (± 5 years) to 2 healthy controls. We collected detailed information on ASCVD diagnosis, anthropometric measurements, demographics (age, education, residency, health insurance, physical activity), blood test results, chronic medication history, and any history of heart failure or sleep apnea. Both classical and novel (emerging) CV risk factors were recorded for all cases and their matched controls. “Urban communities” were defined as communities with high population density, determined by the government as a “city” [15]. On the other hand, “rural society” is any community of people outside the urban settlements.
Definition of ASCVD
ASCVD was defined as the presence of at least one major atherosclerotic condition. These included acute coronary syndrome (STEMI, NSTEMI, or unstable angina), significant epicardial coronary artery disease identified on CCTA (≥ 50% stenosis in the left main artery or ≥ 70% stenosis in any other major coronary vessel), ischemic or hemorrhagic stroke, transient ischemic attack (TIA), extracranial carotid artery disease (ECCAD), or peripheral arterial disease (PAD).
STEMI was defined as ischemic chest pain accompanied by ST elevation (≥ 1.5 mm in leads V2-V3 or ≥ 1 mm in two or more contiguous leads) along with elevated cardiac biomarkers. NSTEMI was characterized by ischemic symptoms with ST depression, T-wave inversion, or even a normal ECG, but with elevated cardiac enzymes. Unstable angina was defined as ischemic chest pain with ECG evidence of ischemia but without biomarker elevation. ECCAD and PAD diagnoses were based on clinical symptoms supported by Doppler studies, CT imaging, or angiographic confirmation of atherosclerosis. Stroke and TIA diagnoses were confirmed by a neurologist and verified with the appropriate neuroimaging.
Classical risk factors
Classical ASCVD risk factors in this study included HTN, smoking, obesity, metabolic syndrome, dyslipidemia, low HDL-C, and T2DM. HTN was defined as systolic BP ≥ 140 mmHg and/or diastolic BP ≥ 90 mmHg on at least 2 occasions or the use of antihypertensive medication. T2DM was diagnosed based on classic hyperglycemic symptoms with random glucose ≥ 200 mg/dl, fasting glucose ≥ 126 mg/dl, HbA1c ≥ 6.5%, or documented history of DM or use of DM medications. Dyslipidemia was defined as LDL-C >70 mg/dl in patients with ASCVD or T2DM, and > 116 mg/dl in others. Low HDL-C was defined as < 50 mg/dl. Obesity was defined as BMI ≥ 30 kg/m². Metabolic syndrome was defined by the presence of 4 components: HTN, obesity, low HDL-C, and hypertriglyceridemia (> 200 mg/dl) at the same time.
Novel risk factors
We also assessed several novel ASCVD risk factors among urban and rural women, including preterm delivery, HDP, GDM, premature menopause, polycystic ovary syndrome (PCOS), and depression. Preterm delivery was defined as birth before 37 weeks’ gestation. HDP included gestational HTN (onset after 20 weeks of pregnancy), chronic HTN, preeclampsia (BP > 140 mmHg with end-organ damage), and eclampsia (seizures following preeclampsia). GDM was defined as glucose intolerance first recognized during pregnancy. PCOS was diagnosed using the Rotterdam criteria (≥ 2 criteria) or prior gynecologic diagnosis [16]. Premature menopause was defined by a prior diagnosis or by oligomenorrhea before age 40 lasting > 4 months with elevated gonadotropins on two tests 4-6 weeks apart. Depression was defined by a documented psychiatric diagnosis or prescribed antidepressant therapy.
Statistical analysis
Descriptive statistics are presented as means with standard deviation (SD) in case of continuous variables, or as frequencies and percentages in case of categorical variables. To compare continuous variables, means were compared using an independent t-test, while categorical variables were compared using the Chi-square test or Fisher’s exact test, as appropriate. Statistical significance was determined when p < 0.05. Statistical analysis was computed using the R Language and Environment for Statistical Computing (version 4.1.2, R Core Team, Vienna, Austria).
Ethical considerations
This observational study was carried out according to the Declaration of Helsinki [17], which was registered in the ClinicalTrials.gov database (NCT04975503). This study obtained ethical approval from an institutional review board at each participating institute in the 3 target regions (approval number IH-IRB-IRC-7-29-2021). In addition, written informed consent was obtained from each patient.
Results
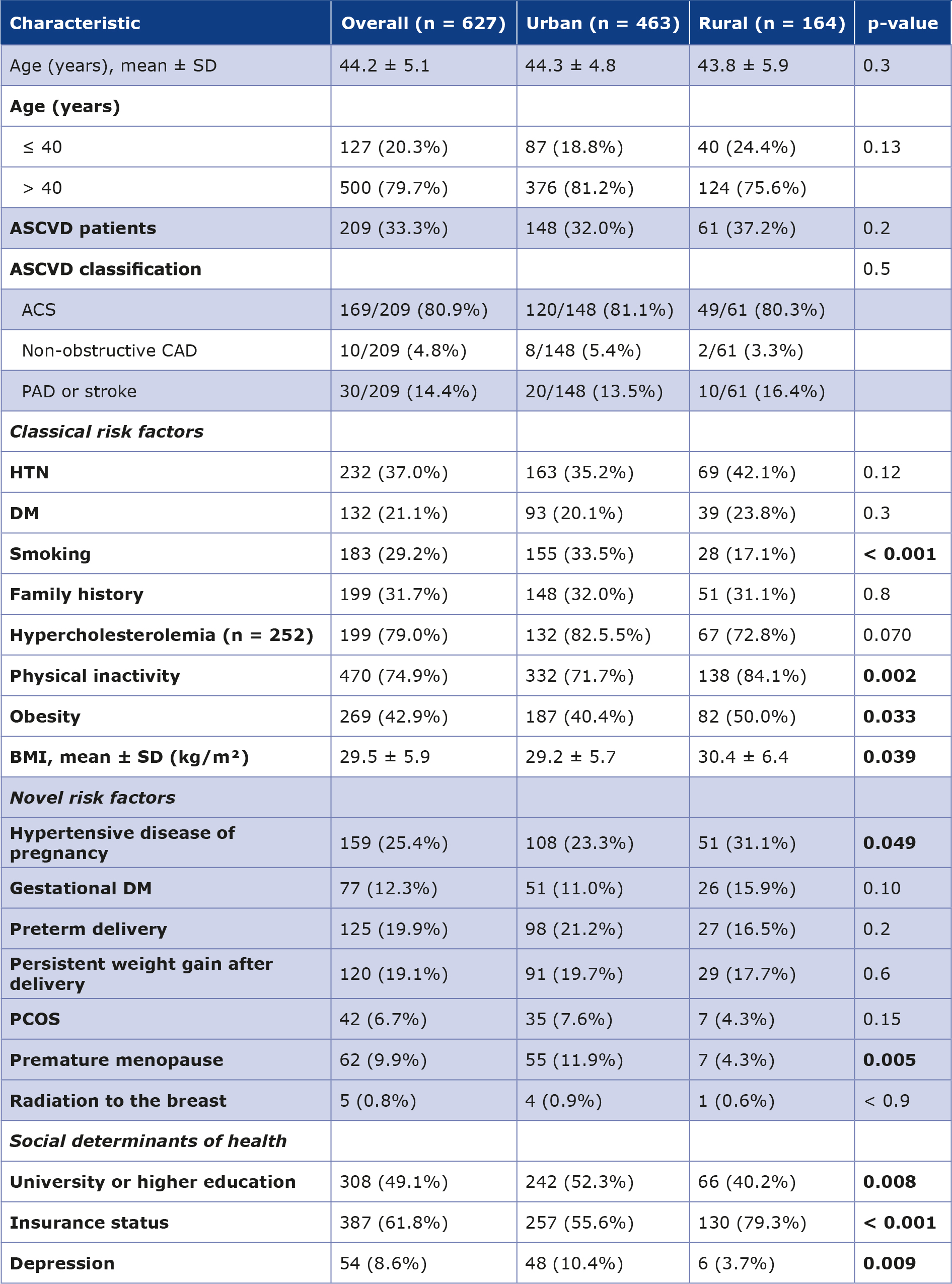
A total of 627 women between 18 and 50 years of age were included in the study, with a mean age of 44.2 ± 5.1 years. Most participants lived in urban areas (73.8%), while 164 of them (26.2%) were residents of rural regions. Baseline demographics, ASCVD prevalence, and CV risk factors by residence type are summarized in Table 1.
Table 1. Demographics, risk factors, and social attributes of young women living in urban vs. rural residence
ACS – acute coronary syndrome, ASCVD – atherosclerotic cardiovascular disease, BMI – body mass index, CAD – coronary artery disease, DM – diabetes mellitus, HTN – hypertension, PAD – peripheral artery disease, PCOS – polycystic ovary syndrome, SD – standard deviation
Age distribution was similar between urban and rural participants, and there was no significant difference in the type of ASCVD diagnosed in the two groups (32.0% vs. 37.2%, p = 0.5). Among the classical risk factors, smoking was more common among urban residents compared to rural residents (33.5% vs. 17.1%, p < 0.001). In contrast, rural residents demonstrated higher rates of physical inactivity and obesity and had a higher mean BMI (p < 0.05). Serum LDL concentrations were available for 252 participants (40.2%). Specifically, hypercholesterolemia was identified in 132 of 160 urban women (82.5%) and 67 of 92 rural women (72.8%), with no statistically significant difference (p = 0.07). HTN, DM, and family history of ASCVD were similar between groups (Figure 1).
Figure 1. Prevalence of classical ASCVD risk factors among urban and rural young women
ASCVD – atherosclerotic cardiovascular disease; DM – diabetes mellitus; HTN – hypertension; *p < 0.05 between groups
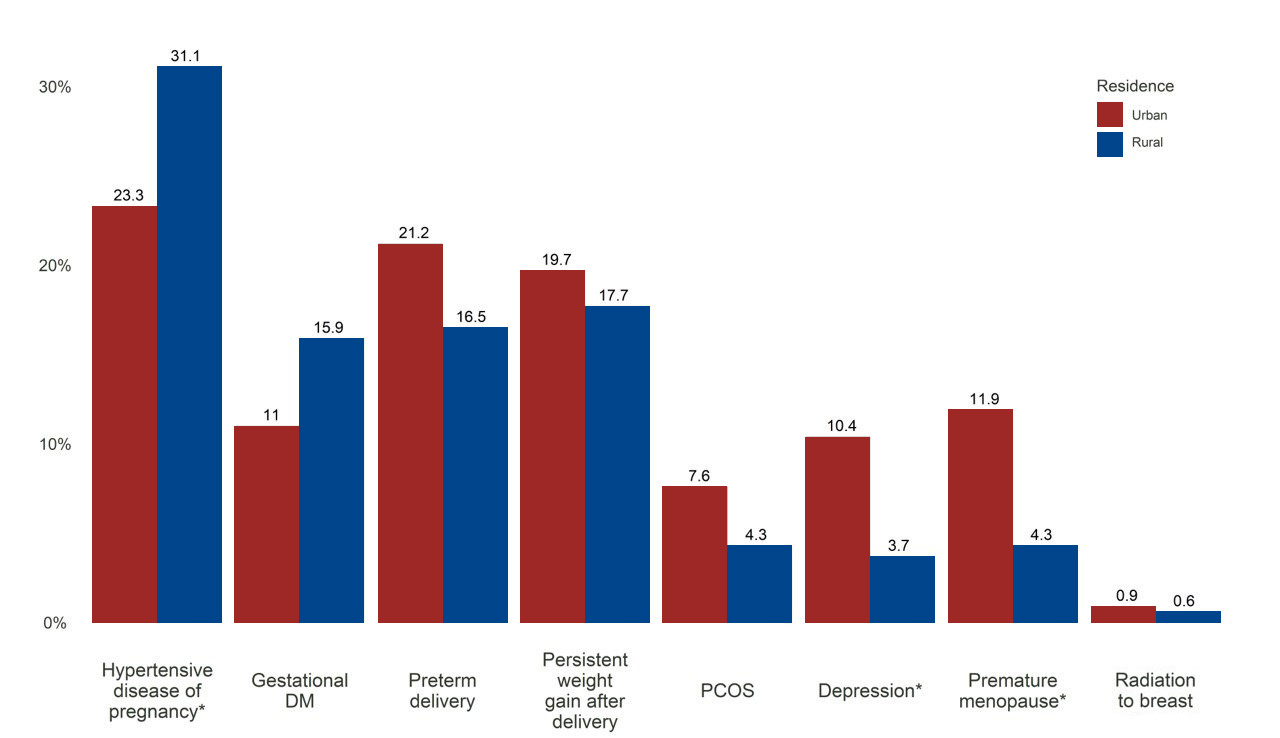
Regarding novel ASCVD risk factors, HDP were more common among rural women. In contrast, depression and premature menopause were significantly more prevalent among urban women. GDM, preterm delivery, persistent postpartum weight gain, PCOS, and prior breast radiation (due to cancer) were comparable between the two groups (p > 0.05) (Figure 2). Additionally, women living in urban areas were more likely to have a university-level or higher education, while being less likely to have health insurance coverage.
Figure 2. Prevalence of novel ASCVD risk factors among urban and rural young women
DM – diabetes mellitus; PCOS – polycystic ovary syndrome; *p < 0.05 between groups
Discussion
In this study, physical inactivity or sedentary lifestyle was the most prevalent classical risk factor among women with an overall percentage of (74.9%) comprising of 71.7% and 84.1% in urban and rural areas’ residents respectively. Our results were consistent with the observations of the 2009 Northern Sweden MONICA cohort [18]. Another study established a positive correlation between sedentary lifestyle and mortality among rural inhabitants in the USA regardless of depressive symptoms [19]. According to the 2019 Jordan National Stepwise Survey (STEPs) for Noncommunicable Disease Risk Factors, 25% of respondents didn’t meet the WHO recommendations for physical activity for health, with an average of (24%) women being physically inactive [2]. Another Jordanian study reported lower prevalence of physical activity practice in women than in men [20]. Such findings of high rural than urban prevalence of inactivity could be related to the deficiency of sporting facilities in addition to the more conservative culture of rural areas than those living in cities. Doctors and other medical care givers should encourage women of any age to engage in regular physical activity, as it reduces the risk of mortality and cardiovascular disease (CVD) events [21]. Similar results were reported by Kazemi et al. [22]. It is worth mentioning the impact of a 10-minute substitution of sedentary time with light-intensity physical activity on all-cause and CVD-specific mortality risk reduction among patients with heart failure [23].
In another study, the prevalence of obesity (BMI ≥ 30) among Jordanian women was higher than those reported in Saudi, Iranian and American women, while similar to that reported among Turkish women [24]. Obesity in our results accounts for an overall prevalence of (42.9%), recording a higher percentage among rural dwellers (50.0%) than in urban (40.4%). The overall mean BMI among our study’s participants was in the overweight range (29.5). Urban residents had a similar mean BMI (29.2), while rural women's mean BMI fell within the obesity range (30.4). In rural areas, women exhibit lower levels of physical activity, often attributed to a higher percentage of women engaged in homemaking duties, in contrast to their urban counterparts. Our findings align with those of the Swedish MONICA study [18], but contradict those reported in India [25].
An overall 29.2% of women in this study reported smoking, with higher percent 33.5% in urban areas versus 17.1% in rural. Such findings could be attributed to the relatively higher incomes and financial prosperity among people living in urban areas compared to rural dwellers. Opposite results with rural predominance were found in India, such different findings could be correlated to the diversity and the wide spread of tobacco products in India, particularly the cheap smokeless tobacco [25]. Whilst our results and the study from India showed urban-rural distribution difference in tobacco consumption, such difference was not observed in the Swedish MONICA study [18]. Medical intervention regarding smoking cessation should be taken into consideration, particularly because females are more prone than males for coronary heart events [26-27].
Contrary to existing literature, our study did not reveal statistically significant urban-rural disparities in the distribution of HTN, DM, and hypercholesterolemia. Such similarity in the distribution of these 3 risk factors could be influenced by the ongoing process of urbanization within rural communities and the substantial migration rates of rural residents to urban areas. This socio-economic situation may contribute to a convergence in health profiles between urban and rural populations, blurring traditional distinctions.
A 2019 study conducted in Jordan revealed that almost one-third of Jordanian adults had HTN [28]. We noted a similar distribution of HTN among the urban rural groups of our study cohort, which is in contrast to the findings of the Swedish MONICA study, where rural dwellers reported higher burden of increased systolic blood pressure in both men and women [18].
DM is a global health problem which besides end-organ damage also causes and accelerates atherosclerotic CV events [29]. Similar urban-rural distribution was noted by a study in India [25] and the Swedish MONICA [18] which consists with our findings. A Chinese study discussed sex and urban-rural distribution difference of dyslipidemia, revealed higher percentages of dyslipidemia (apart from low HDL-C) in rural residents with females exhibiting higher whole lipid profile readings compared to males in both areas of residence contrasting to our results [30]. Higher education in the Arab world is rapidly evolving, shaped by the diverse cultural and socio-economic contexts of the 22 countries in the MENA [31]. Higher level of education is inversely linked to smoking and high salt intake on the one hand, while positively linked to increase in physical activity on the other hand, as both of these lifestyle habits may provide a clue for such a relationship [32]. In our study, nearly half of the participants (49.1%) had higher education. Women in urban areas r eported a higher prevalence of higher education (52.3%) compared to their rural counterparts (40.2%). These numbers are not so different as the mean age of most participants in both groups is quite high.
As for the novel ASCVD risk factors, HDP (including pre-eclampsia, gestational HTN and eclampsia) are common complications of pregnancy globally and are the top causes of maternal and fetal morbidity and mortality [32]. In 2017, the incidence of preeclampsia in Jordan was approximately 1.5%, which was similar to the other countries in the region [33]. In our study, we found that there is a significant difference in the prevalence of HDP between urban and rural residents, with a p-value of 0.049. The difference was more obvious among rural participants, where 31.1% were affected compared to 23.4% of their urban counterparts. Similarly, a study conducted in South Africa revealed that most of the women with HTN over the age of 65 were living in rural areas [34]. This variability in prevalence might be explained by the variety of maternal risk factors, including age, parity, obesity, high blood pressure and the region.
Depression is a well-established independent risk factor for CVD in the non-pregnant population. However, the risk of a new CVD diagnosis diagnosed postpartum was elevated among patients with prenatal depression [35]. A Swedish nationwide study demonstrated that the risk of developing CVD varies between women with antepartum depression (APD) and postpartum depression (PPD), with higher risk among women with PPD [36]. We found a significant difference in depression prevalence (p = 0.009) between women living in urban (n = 48, 10.4%) and rural (n = 6, 3.7%) areas. A study conducted on the prevalence of depression and mood disorders among African American women and non-Hispanic white women revealed that rural residence is linked to lower rates of depression: because these women have developed resources and coping mechanisms to deal with stressful circumstances (including supportive social ties and high levels of religious participation) [37].
The American College of Cardiology (ACC) and American Heart Association (AHA) guidelines have demonstrated that premature menopause (at > 40 years of age) might pose as a risk for ASCVD due to the cardiometabolic changes that occur earlier [38]. A 2023 study of a large Korean cohort found that premature menopause was associated with 1.5 times greater risk of MI, 1.25 times risk of ischemic stroke, and 1.2 times the risk of all-cause mortality when compared to women with normal menopause [39]. In our study, 62 women had premature menopause, 55 of them were living in urban areas (11.9%), and 7 were in rural (4.3%), p = 0.005. This difference is consistent with the findings of an Indonesian study, that revealed women living in rural areas lowered their potential for premature menopause by 0.67 times compared to women who live in urban areas, who are 1.46 times more likely to experience premature menopause [40].
Limitations
It is important to acknowledge several limitations that may have influenced the interpretation and generalizability of our findings. The small sample size in this study may have limited the ability to draw definitive conclusions and generalize the findings to broader populations. Furthermore, the limited availability of resource data for comparison with other studies restricted our ability to assess the study.
Our findings study underscore the critical need for sex-specific approaches in CV care. Recent international collaborations have emphasized the necessity of timely management of acute coronary syndrome in women to improve their prognosis which often is worse compared to men [41]. Furthermore, the establishment of specialized heart centers for women has been proposed as a vital modality to enhance long-term CV, metabolic, and reproductive care, offering a comprehensive solution to the regional disparities identified in our cohort [42].
Conclusions
Our cohort demonstrated clear differences in ASCVD risk factor patterns between urban and rural women in Jordan and Gaza. Urban participants showed worse overall clinical profiles, with higher rates of premature menopause, depression, and smoking, whereas hypertensive disorders of pregnancy emerged as the most significant novel risk factor among rural women. Physical inactivity and obesity were also more common in rural areas. Other classical risk factors showed no significant differences. Our findings highlight the need for population-specific strategies addressing both classical and novel ASCVD risk factors.
Funding
The authors relied on self-financing sources to complete the preparation and publication of their research article.
Conflict of interest
All authors assure that there is no conflict of interest with any party and that the research was prepared within the scientific methodology that does not contain sensitive personal data or conflict with the interest of any party.
References
| 1. |
Benjamin EJ, Blaha MJ, Chiuve SE, Cushman M, Das SR, Deo R, et al. Heart Disease and Stroke Statistics –2017 Update: A Report From the American Heart Association. Circulation [Internet]. 2017;135(10). Available from: https://www.ahajournals.org/doi/10.1161/CIR.0000000000000485.
|
| 2. |
Jaber S. Jordan National Stepwise Survey (STEPs) for Noncommunicable Diseases Risk Factors 2019 [Internet]. 2019 STEPS Country Report Jordan. Ministry of Health, Jordan; 2020. 1–118 p. Available from: https://www.who.int/publications/m/item/2019-steps-country-report-jordan.
|
| 3. |
Alhuneafat L, Ta’ani O Al, Jabri A, Tarawneh T, ElHamdan A, Naser A, et al. Cardiovascular disease burden in the Middle East and North Africa region. Curr Probl Cardiol [Internet]. 2024;49(3):102341. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0146280623007582.
|
| 4. |
Dewan P, Rørth R, Jhund PS, Shen L, Raparelli V, Petrie MC, et al. Differential Impact of Heart Failure With Reduced Ejection Fraction on Men and Women. J Am Coll Cardiol [Internet]. 2019;73(1):29–40. Available from: http://www.ncbi.nlm.nih.gov/pubmed/30621948.
|
| 5. |
Parapid B. Cardiovascular risk in women: here, there and everywhere. Eur J Transl Clin Med [Internet]. 2025;8(2):5–8. Available from: https://ejtcm.gumed.edu.pl/articles/208813.
|
| 6. |
Vogel B, Acevedo M, Appelman Y, Bairey Merz CN, Chieffo A, Figtree GA, et al. The Lancet women and cardiovascular disease Commission: reducing the global burden by 2030. Lancet [Internet]. 2021;397(10292):2385–438. Available from: https://doi.org/10.1016/S0140-6736(21)00684-X.
|
| 7. |
Xu X, Bao H, Strait KM, Edmondson DE, Davidson KW, Beltrame JF, et al. Perceived Stress After Acute Myocardial Infarction: A Comparison Between Young and Middle-Aged Women Versus Men. Psychosom Med [Internet]. 2017;79(1):50–8. Available from: https://journals.lww.com/00006842-201701000-00007.
|
| 8. |
Alawadi F, Assaad-Khalil SH, Almahmeed W, Alamuddin N, Alkandari H, Haddad JA, et al. 21-LB: Prevalence of Atherosclerotic Cardiovascular Diseases in Women with Type 2 Diabetes across the Middle East and Africa — Primary Gender Analysis of the PACT-MEA Study. Diabetes [Internet]. 2023;72(Supplement_1). Available from: https://diabetesjournals.org/diabetes/article/72/Supplement_1/21-LB/149270/21-LB-Prevalence-of-Atherosclerotic-Cardiovascular.
|
| 9. |
Lamprea-Montealegre JA, Zelnick LR, Hall YN, Bansal N, de Boer IH. Prevalence of Hypertension and Cardiovascular Risk According to Blood Pressure Thresholds Used for Diagnosis. Hypertension [Internet]. 2018;72(3):602–9. Available from: https://www.ahajournals.org/doi/10.1161/HYPERTENSIONAHA.118.11609.
|
| 10. |
Wenger NK, Arnold A, Bairey Merz CN, Cooper-DeHoff RM, Ferdinand KC, Fleg JL, et al. Hypertension Across a Woman’s Life Cycle. J Am Coll Cardiol [Internet]. 2018;71(16):1797–813. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0735109718333126.
|
| 11. |
Yusuf S, Hawken S, Ôunpuu S, Dans T, Avezum A, Lanas F, et al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): case-control study. Lancet [Internet]. 2004;364(9438):937–52. Available from: https://doi.org/10.1016/S0140-6736(04)17018-9.
|
| 12. |
Wahrenberg A, Kuja‐Halkola R, Magnusson PKE, Häbel H, Warnqvist A, Hambraeus K, et al. Cardiovascular Family History Increases the Risk of Disease Recurrence After a First Myocardial Infarction. J Am Heart Assoc [Internet]. 2021;10(23). Available from: https://www.ahajournals.org/doi/10.1161/JAHA.121.022264.
|
| 13. |
Theodorou A, Karagiannakis DS, Stefanaki K, Kassi E, Peppa M, Vryonidou A, et al. Female-specific risk factors for cardiovascular disease: an update. Hormones (Athens) [Internet]. 2024;23(4):637–53. Available from: http://www.ncbi.nlm.nih.gov/pubmed/38922384.
|
| 14. |
Hammoudeh AJ, Jallad M, Khader Y, Badaineh Y, Tabbalat RA, Zammar H, et al. Atherosclerotic Cardiovascular Disease Novel and Traditional Risk Factors in Middle Eastern Young Women. The ANCORS-YW Study. Glob Heart [Internet]. 2024;19(1):59. Available from: http://www.ncbi.nlm.nih.gov/pubmed/39035774.
|
| 15. |
Sclar ED, Volavka-Close N. Urban Health: an Overview ED 2021. Elsevier BV; 2020.
|
| 16. |
Hmoud TR, Jawad MM, Alredha RDA. Hormonal profiles and the diagnostic utility of serum dihydrotestosterone in polycystic ovary syndrome: a comparative case-control study. Eur J Transl Clin Med [Internet]. 2025;8(2):17–24. Available from: https://doi.org/10.31373/ejtcm/208403.
|
| 17. |
World Medical Association. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA [Internet]. 2013;310(20):2191–4. Available from: https://pubmed.ncbi.nlm.nih.gov/24141714/.
|
| 18. |
Lindroth M, Lundqvist R, Lilja M, Eliasson M. Cardiovascular risk factors differ between rural and urban Sweden: the 2009 Northern Sweden MONICA cohort. BMC Public Health [Internet]. 2014;14(1):825. Available from: https://bmcpublichealth.biomedcentral.com/articles/10.1186/1471-2458-14-825.
|
| 19. |
Park LG, Dracup K, Whooley MA, McCulloch C, Lai S, Howie-Esquivel J. Sedentary lifestyle associated with mortality in rural patients with heart failure. Eur J Cardiovasc Nurs [Internet]. 2019;18(4):318–24. Available from: https://academic.oup.com/eurjcn/article/18/4/318-324/5925232.
|
| 20. |
Barghouti F, Jaghbir M, Aburmaileh N, Jallad D, Qudah Y. Leisure Time Physical Activity in Jordan: Knowledge and Sociodemographic Determinants. Int Med J [Internet]. 2015 1;22:183–287. Available from: https://www.researchgate.net/publication/281740602_Leisure_Time_Physical_Activity_in_Jordan_Knowledge_and_Sociodemographic_Determinants.
|
| 21. |
Lear SA, Hu W, Rangarajan S, Gasevic D, Leong D, Iqbal R, et al. The effect of physical activity on mortality and cardiovascular disease in 130 000 people from 17 high-income, middle-income, and low-income countries: the PURE study. Lancet [Internet]. 2017;390(10113):2643–54. Available from: https://doi.org/10.1016/S0140-6736(17)31634-3.
|
| 22. |
Kazemi A, Soltani S, Aune D, Hosseini E, Mokhtari Z, Hassanzadeh Z, et al. Leisure-time and occupational physical activity and risk of cardiovascular disease incidence: a systematic-review and dose-response meta-analysis of prospective cohort studies. Int J Behav Nutr Phys Act [Internet]. 2024;21(1):45. Available from: https://ijbnpa.biomedcentral.com/articles/10.1186/s12966-024-01593-8.
|
| 23. |
Kim Y, Canada JM, Kenyon J, Billingsley HE, Arena R, Lavie CJ, et al. Effects of Replacing Sedentary Time With Physical Activity on Mortality Among Patients With Heart Failure: National Health and Nutrition Examination Survey Follow-Up Study. Mayo Clin Proc [Internet]. 2022;97(10):1897–903. Available from: https://doi.org/10.1016/j.mayocp.2022.05.009.
|
| 24. |
Khader Y, Batieha A, Ajlouni H, El-Khateeb M, Ajlouni K. Obesity in Jordan: prevalence, associated factors, comorbidities, and change in prevalence over ten years. Metab Syndr Relat Disord [Internet]. 2008;6(2):113–20. Available from: http://www.ncbi.nlm.nih.gov/pubmed/18510436.
|
| 25. |
Behera S, Sharma R, Yadav K, Chhabra P, Das M, Goel S. Prevalence and predictors of risk factors for cardiovascular diseases among women aged 15–49 years across urban and rural India: findings from a nationwide survey. BMC Womens Health [Internet]. 2024;24(1):77. Available from: https://bmcwomenshealth.biomedcentral.com/articles/10.1186/s12905-023-02869-0.
|
| 26. |
Huxley RR, Woodward M. Cigarette smoking as a risk factor for coronary heart disease in women compared with men: a systematic review and meta-analysis of prospective cohort studies. Lancet [Internet]. 2011;378(9799):1297–305. Available from: https://doi.org/10.1016/S0140-6736(11)60781-2.
|
| 27. |
King A. Risk factors: Cigarette smoking increases the risk of coronary heart disease in women more than in men. Nat Rev Cardiol [Internet]. 2011;8(11):612. Available from: http://www.ncbi.nlm.nih.gov/pubmed/21878881.
|
| 28. |
Khader Y, Batieha A, Jaddou H, Rawashdeh SI, El-Khateeb M, Hyassat D, et al. Hypertension in Jordan: Prevalence, Awareness, Control, and Its Associated Factors. Int J Hypertens [Internet]. 2019;2019:3210617. Available from: http://www.ncbi.nlm.nih.gov/pubmed/31186953.
|
| 29. |
Global report on diabetes [Internet]. 2016. Available from: https://www.who.int/publications/i/item/9789241565257.
|
| 30. |
Opoku S, Gan Y, Fu W, Chen D, Addo-Yobo E, Trofimovitch D, et al. Prevalence and risk factors for dyslipidemia among adults in rural and urban China: findings from the China National Stroke Screening and prevention project (CNSSPP). BMC Public Health [Internet]. 2019;19(1):1500. Available from: https://bmcpublichealth.biomedcentral.com/articles/10.1186/s12889-019-7827-5.
|
| 31. |
Altbach PG, Reisberg L, Rumbley LE. Trends in Global Higher Education: Tracking an Academic Revolution. A Report Prepared for the UNESCO 2009 World Conference on Higher Education [Internet]. Paris: UNESCO; 2009. Available from: https://unesdoc.unesco.org/ark:/48223/pf0000183168.
|
| 32. |
Hu M, Yang T, Yang Y. Causal Associations of Education Level With Cardiovascular Diseases, Cardiovascular Biomarkers, and Socioeconomic Factors. Am J Cardiol [Internet]. 2024;213:76–85. Available from: https://doi.org/10.1016/j.amjcard.2023.06.044.
|
| 33. |
Khader YS, Batieha A, Al-Njadat RA, Hijazi SS. Preeclampsia in Jordan: incidence, risk factors, and its associated maternal and neonatal outcomes. J Matern Fetal Neonatal Med [Internet]. 2018;31(6):770–6. Available from: http://www.ncbi.nlm.nih.gov/pubmed/28274172.
|
| 34. |
Mphekgwana PM, Malema N, Monyeki KD, Mothiba TM, Makgahlela M, Kgatla N, et al. Hypertension Prevalence and Determinants among Black South African Adults in Semi-Urban and Rural Areas. Int J Environ Res Public Health [Internet]. 2020;17(20). Available from: http://www.ncbi.nlm.nih.gov/pubmed/33066410.
|
| 35. |
Ackerman‐Banks CM, Lipkind HS, Palmsten K, Pfeiffer M, Gelsinger C, Ahrens KA. Association of Prenatal Depression With New Cardiovascular Disease Within 24 Months Postpartum. J Am Heart Assoc [Internet]. 2023;12(9):e028133. Available from: https://doi.org/10.1161/JAHA.122.028133.
|
| 36. |
Lu D, Valdimarsdóttir UA, Wei D, Chen Y, Andreassen OA, Fang F, et al. Perinatal depression and risk of maternal cardiovascular disease: a Swedish nationwide study. Eur Heart J [Internet]. 2024;45(31):2865–75. Available from: https://academic.oup.com/eurheartj/article/45/31/2865/7693155.
|
| 37. |
Weaver A, Himle JA, Taylor RJ, Matusko NN, Abelson JM. Urban vs Rural Residence and the Prevalence of Depression and Mood Disorder Among African American Women and Non-Hispanic White Women. JAMA psychiatry [Internet]. 2015;72(6):576–83. Available from: http://www.ncbi.nlm.nih.gov/pubmed/25853939.
|
| 38. |
Torbati T, Shufelt C, Wei J, Noel Bairey Merz C. Premature menopause and cardiovascular disease: can we blame estrogen? Eur Heart J [Internet]. 2022;43(40):4158–60. Available from: http://www.ncbi.nlm.nih.gov/pubmed/36239222.
|
| 39. |
Lee GB, Nam GE, Kim W, Han B, Cho KH, Kim SM, et al. Association Between Premature Menopause and Cardiovascular Diseases and All-Cause Mortality in Korean Women. J Am Heart Assoc [Internet]. 2023;12(22):e030117. Available from: http://www.ncbi.nlm.nih.gov/pubmed/37947103.
|
| 40. |
Leone T, Brown L, Gemmill A. Secular trends in premature and early menopause in low-income and middle-income countries. BMJ Glob Heal [Internet]. 2023;8(6):e012312. Available from: https://doi.org/10.1136/bmjgh-2023-012312.
|
| 41. |
Manzo-Silberman S, Hawranek M, Banerjee S, Kaluzna-Oleksy M, Alasnag M, Paradies V, et al. Call to action for acute myocardial infarction in women: international multi-disciplinary practical roadmap. Eur Hear J open [Internet]. 2024;4(6):oeae087. Available from: http://www.ncbi.nlm.nih.gov/pubmed/39507804.
|
| 42. |
Parapid B, Kanjuh V, Kostic V, Polovina S, Dinic M, Loncar Z, et al. Women’s health in Serbia - past, present, and future. Srp Arh Celok Lek [Internet]. 2021;149(11–12):745–54. Available from: https://doiserbia.nb.rs/Article.aspx?ID=0370-81792100105P.
|
