


Effects of HRV biofeedback training on recovery, stress management, reaction time and concentration in competitive rowing – preliminary study


Abstract
Background: Our aim was to determine the effect of HRV biofeedback (HRVB) training on psychophysiological factors, e.g. reaction time, stress management and concentration during the starting period in competitive rowing.
Material and methods: 12 senior national team rowers aged 20-40 (both men and women) were assigned to an experimental (n = 6) and a control (n = 6) group. The experimental group performed HRVB training for 4 weeks, for 20 minutes, twice a day. The control group did not perform any respiratory training. Parameters such as reaction time, resting breathing rate, concentration, subjective stress and heart rate variability were evaluated during the pre-test, post-test and post-post test phases.
Results: We noted an improvement in reaction time in the experimental group after HRVB training (pre-test 63.8 sec to post-post test 58.8 sec) and no significant statistical differences in the control group, as well as a statistically significant reduction in resting respiratory rate frequency in the experimental group in comparison to the control group in the post-test (p = 0.0398). Other analyses did not exceed the threshold for statistical significance.
Conclusions: Our results suggest that HRVB training may reduce the resting respiratory rate in the experimental group and may improve the reaction time of rowers.
Citation
Myszka Z, Wolff M, Basta P, Kozłowski D. Effects of HRV biofeedback training on recovery, stress management, reaction time and concentration in competitive rowing – preliminary study. Eur J Transl Clin Med. 2025;8(1):32-44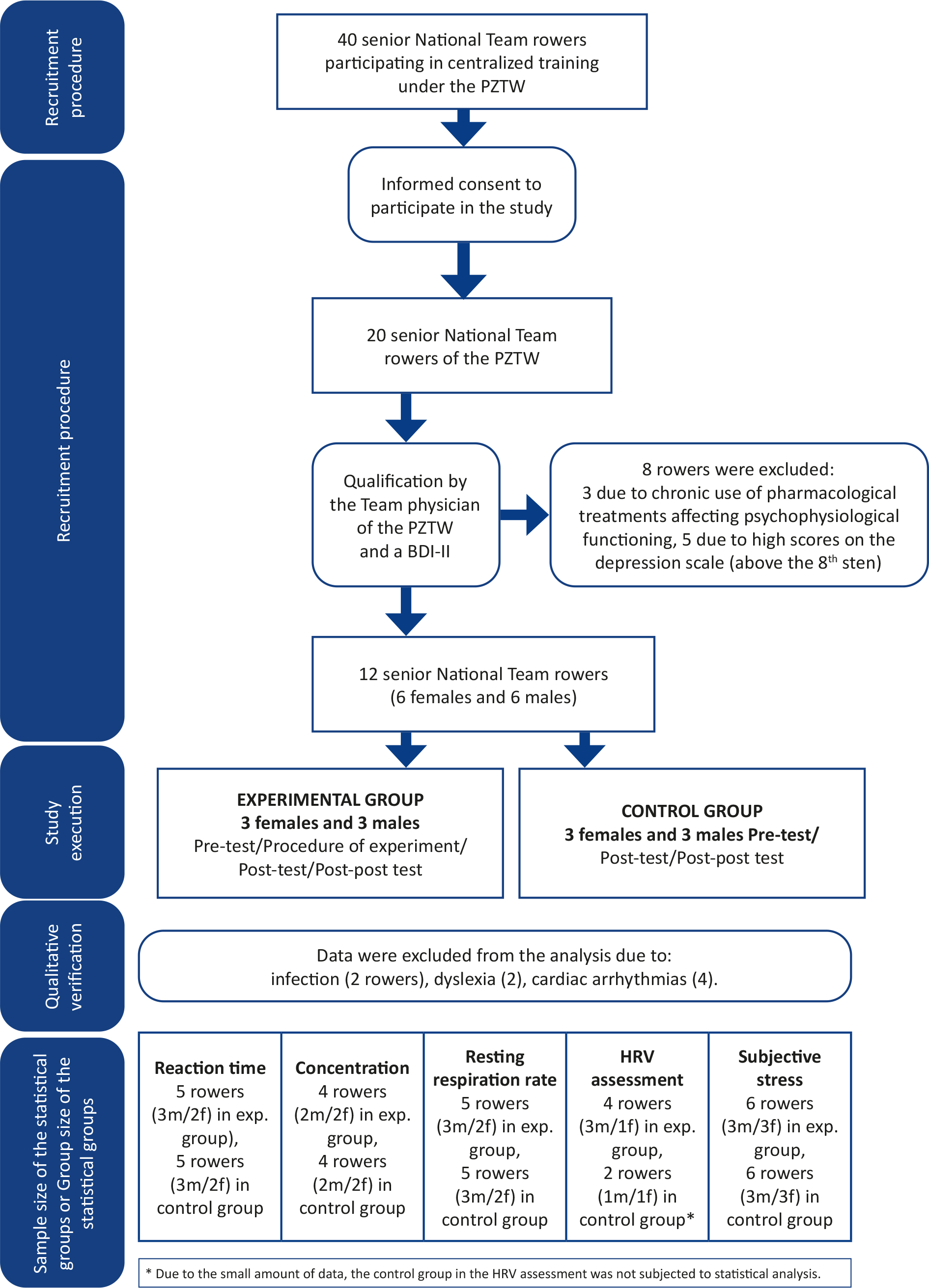











Abbreviations
- HRV – heart rate variability
- HRVB – heart rate variability biofeedback
- BDI-II – Beck Depression Inventory – 2nd Edition
- TUS – Attention and Perceptiveness Tests
- SDNN – standard deviation of RR intervals
- RMSSD – root mean square of successive RR interval differences
- HR – heart rate
- LF – low frequency
- HF – high frequency
- VO2 – max – maximum oxygen uptake
- PZTW – Polish Federation of Rowing Associations
Introduction
Rowing is largely an endurance sport and requires athletes to have highly developed skills to manage their mental and physical resources. The development of peak physical performance continues to evolve as new insights emerge from the field of human physiology. This domain encompasses a broad range of topics from nutrition science (e.g. the effects of caffeine intake on rowing performance), to exercise physiology (e.g. the impact of kettlebell training on muscular strength and endurance of rowers) [1-2]. Furthermore, recent research explores more specific interventions, such as the effects of blood flow restriction on power output during the start phase, heart rate (HR), and systemic acidosis [3].
In contrast, the level of knowledge and its practical application in research and training aimed at enhancing the psychophysiological and mental skills of rowers remains considerably underdeveloped. A review of the available literature revealed no studies investigating the Polish senior elite rowing population with respect to the assessment of mental skills (e.g. focus, reaction time) or stress levels. Existing publications are limited to research on stress responses, primarily examining cortisol fluctuations in relation to varying training intensities, or studies exploring changes in antioxidant defense systems in young rowers following an annual training cycle [4-5].
Moreover, no research was identified concerning the effects of heart rate variability biofeedback (HRVB) training in the context of Polish sport. Considering the fact that competitive rowing demands years of training and sacrifice (often leading to overuse of the body and injuries), simple and effective tools to reduce fatigue levels or to accelerate the recovery seems to be the basis of modern training [6].
One of the analyses of the psychophysiological state, depicting the body’s ability to determine stress levels and regulatory capacity, is the analysis of HRV [7]. A high HRV is a sign that the heart is healthy since it has more flexibility to react to stressors (physiological or environmental) [8]. From a practical point of view, it remains to be determined if it can also be used as a predictor of athletic condition and of athletic achievements [9]. Cardiovascular functions (including the HRV rate) are regulated by the autonomic nervous system, which via sympathetic and parasympathetic innervation of the blood vessels, directly modifies vascular wall tension and influences cardiac function [10].
However, humans are able to influence their own HRV by using breathing training. One such method is HRVB training. Biofeedback acutely increased both HRV and baroreflex gain, and chronically increased baroreflex gain and peak expiratory flow even among healthy individuals, in whom these measures ordinarily are thought to be stable [11]. Moreover, breathing at this frequency causes an increase or decrease in heart rate depending on the phase of breathing, maximizing the efficiency of gas exchange and affecting the efficiency of the body. HRVB is used to treat a number of diseases and ailments, such as asthma, pain, depression), hypertension or anxiety [12-16].
A growing number of studies conducted abroad are emerging describing the effects of respiratory training on the performance of athletes in various fields. It has been shown that HRVB training can help train stressed athletes to gain control over their psychophysiological processes, thus helping them achieve maximum performance [17]. In addition, HRVB can produce significant benefits in autonomic markers and anxiety levels in young athletes [18]. Also, it is associated with increased HRV and improved subjective training performance in elite female athletes [19]. Furthermore, HRVB training improved HRV parameters and reduced the number of strokes to complete a virtual 18-hole game of golf (46 strokes in the pre-test, 30 in the posttest) in a group of female golf coaches [20]. Finally, it significantly reduced race time in an experimental group, and reduced skin conductance and increased VO2 max in male and female long-distance running groups [21]. Although research on HRVB training in sports is limited, it suggests that it is a safe, accessible and effective method that appears to offer tangible performance benefits for both athletes and coaches [22].
Rowing races commence with an auditory signal, and subsequently athletes must react swiftly and maintain synchronized oar movements and sustained focus throughout the race. Therefore, our aim was to address the following research question: “does HRVB training influence psychological factors critical to rowing performance (both at the start of and during the race itself) such as reaction time and athlete concentration?”. We also attempted to determine the subjectively perceived stress levels of athletes, along with HRV parameters, and investigate the impact of HRVB breathing training (with resonant frequency individually selected for each athlete) on these factors, as well as its effect on the regulation of the autonomic nervous system (e.g. the resting respiratory rate).
Materials and methods
In 2022, 40 senior athletes from the Polish National Rowing Team, participating in centralized training under the PZTW, were invited to take part in a research project. Twenty athletes provided written informed consent to participate in the study. Following a medical consultation with the Team physician and a psychological assessment for depressive symptoms (21 questions, no time limit) an additional 8 rowers were excluded from the study. Five athletes scored above the threshold sten score of 8 on BDI-II, and 3 were undergoing pharmacological treatment that could potentially affect HRV outcomes.
The inclusion criteria were: the athlete’s appointment to the National Senior Team of the PZTW and voluntary consent to participate in the project. The exclusion criteria were: having a chronic disease and taking medications that have a significant effect on HRV and obtaining a high sten score (< 8 sten) in the BDI-II psychological test.
Based on the recruitment procedure, and the inclusion and exclusion criteria, 6 women and 6 men were selected and randomly assigned to 2 equal groups:
1) The experimental group received HRVB training (3 females and 3 males).
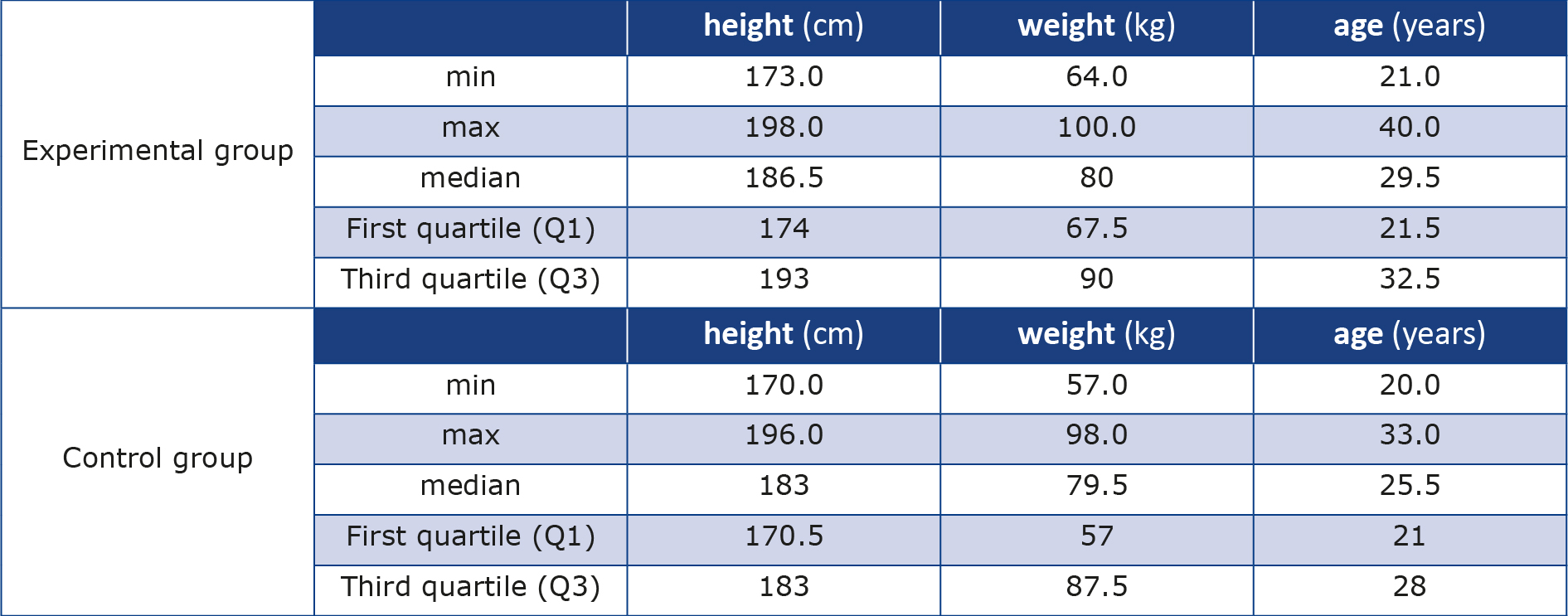
2) The control group did not receive any training (3 females and 3 males) (Table 1).
Table 1. Demographic data
Both groups demonstrated an equivalent elite athletic level within Olympic disciplines. Specifically, 4 athletes in both the experimental and control groups held the International Master Class designation, which denotes having achieved at least a medal at the World and/or European Championships, or having reached the finals or secured a medal at the Olympic Games. Additionally, 2 athletes from each group held the National Master Class designation, having reached the finals of the World and/or European Championships and/ or won a medal at the Polish National Championships. The recruitment data and selection process throughout the project is depicted in Figure 1. The execution stage included the following phases: pre-test, experimental procedure, post-test, and post-post test (Table 2). The next stage of quality verification included ECG analysis by a sports cardiologist, a consultation with the team physician of the PZTW regarding any infection acquired during the post-test period, and interviews to assess the presence of dyslexia. At this stage the presence of cardiac arrhythmias (in at least one of the HRV assessment recordings) was confirmed in 4 individuals, a severe infection in two athletes (1 from the experimental group and 1 from the control group) during the post-test period, and confirmation of a dyslexia diagnosis in 2 athletes (1 from the experimental group and 1 from the control group).
Figure 1. Flowchart of study selection
BDI-II – Beck Depression Inventory 2nd Edition, f – females, m – males, PZTW – Polish Federation of Rowing Associations
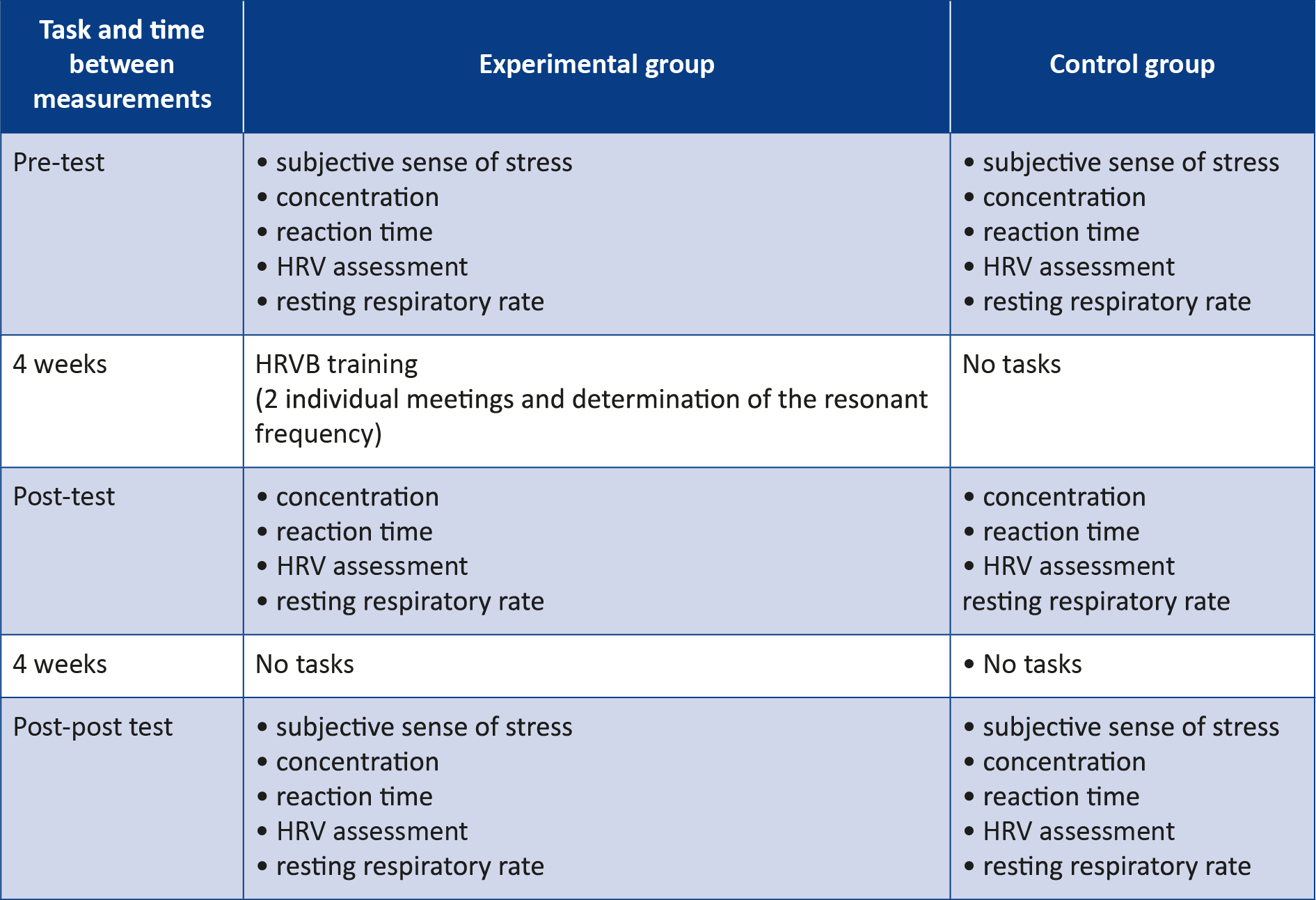
Table 2. Execution stage: tasks and measurements
The results of athletes with confirmed infection were excluded from the statistical analysis of tests that required an optimal physiological condition (e.g. reaction time, concentration test, resting respiratory rate and HRV assessment). Additionally, the results of the 2 athletes with dyslexia were excluded from the statistical analysis of the concentration test. The subjective stress level measurements were conducted both during the pre-test and the control phase, therefore we included the results from all 12 participants in this analysis. The sample sizes of the subgroups included in the final statistical analyses are presented in Figure 1.
This study was conducted in accordance with established ethical standards, including ensuring the safety of participants. All individuals were informed of the purpose and procedures of the study, provided written informed consent, and were made aware of the benefits of participation as well as their right to withdraw at any stage of the study. These procedures adhered to the principles outlined in the European Convention on Bioethics of the Council of Europe. The research was assigned the consent number of the bioethics committee at the Regional Medical Council in Gdansk No. KB-25/24.
Equipment
The measurements were carried out using the following equipment: ECG electrodes (EK-S 45 PSG, Sorimex, Poland), reaction time apparatus (Rox Pro retention lights, A-Champs Ltd., Hong Kong), a coder for HRV assessment and HRVB training (ProComp Infiniti 5.0, Thought Technology Ltd., Canada), and psychological tests such as the BDI-II and TUS, purchased from the Polish Psychological Association [23-24].
Protocols for concentration and subjective stress tests
Concentration tests were conducted using the TUS test, which consisted of crossing out rows of numbers or letters indicated in the test at the highest possible pace within a 3-minute time limit. The raw scores for the speed-of-work indicator were related to the standard sten for a group of soldiers.
Subjective feelings of stress were assessed using a 5-point Likert scale, where 1 indicated a high level of subjectively perceived stress and 5 indicated a low level. Both measurements were taken both at the pretest and at the post-post test stage.
Protocol for time reaction
Time reaction was measured in the pre-test, posttest and post-post test. The procedure included 2 measurements; the second trial was the outcome of a task. It consisted of turning off a randomly switched on light as quickly as possible on one of three cubes placed on a table in front of the contestant. The cubes were placed symmetrically at twenty-centimeter intervals.
Protocol for HRV, resting breathing frequency and HRVB training
HRV, resting breathing frequency measurements and HRVB training were conducted in a quiet, darkened room. Each measurement was preceded by a 10-minute rest period, during which the athlete remained in the supine position. Following this period, a 6-minute ECG recording was obtained in the same position using a single-lead ECG, as well as a respiratory sensor positioned at the level of the athlete’s navel. The HRVB training protocol consisted of two phases conducted within two days: the determination of the individual resonant frequency according to a modified version of the Lehrer protocol and a self-guided training session performed at the prescribed frequency [25]. HRVB training was conducted in the supine position, during which participants followed a visual cue – a dot moving on the screen, rising during inhalation and falling during exhalation at different respiratory rates for about two minutes (6.5, 6.0, 5.5, 5.0 and 4.5 breaths per minute).
During the HRVB training we utilized a respiratory sensor strap and single-lead ECG electrodes. The system continuously displayed the heart rate alongside a real-time spectral analysis of the interbeat interval, recalculated every second using a 30-60 second rolling window. This setup enabled continuous observation of the phase relationship between respiration and HRV. The resonant frequency was determined based on the convergence of several physiological indicators: optimal phase synchrony between heart rate variability and respiration, the highest peak-to-trough amplitude, the highest low frequency (LF) power, a clear and high-amplitude LF peak in the spectral analysis, and a stable “envelope” of the HR curve. The respiratory rate that exhibited the greatest concentration of these features was identified as the participant’s individual resonant frequency, which was then used as the target breathing rate during HRVB training. HRVB training consisted of two 20-minute daily breathing sessions, performed at the individual resonant frequency, supported by mobile breathing applications such as Prana Breath or Breathwork Pacer. Athletes documented their training duration in a personal training diary. During the month preceding the post-post test, participants in the experimental group were instructed to discontinue HRVB training.
Statistical analysis
All procedures in the project included the following dimensions: the mean time to extinguish the randomly switched-on retention light (measured in seconds), concentration – speed of work (stens), resting respiratory rate (rated on a 1-5 scale, where 1 indicates high stress and 5 low stress), HRV – mean RR (beats per minute, BPM), SDNN (ms), RMSSD (ms), HR max-min (BPM), LF power (ms2), high frequency (HF) power (ms2), LF/HF ratio.
For each parameter, four types of statistical result presentations were performed:
1) A descriptive statistical analysis including value distributions, presented as median (1st and 3rd quartiles) and minimum–maximum values, was conducted for each individual measurement.
2) A statistical analysis between measurements. P-values were calculated for the following comparisons: measurement 1 vs. 2, 2 vs. 3, and 1 vs. 3 – separately for the experimental and control groups.
Additionally, adistribution plot of the values for each parameter was generated for the control and experimental groups across the three measurement points. In each plot, the central square represents the median, the boxes indicate the interquartile range (25th to 75th percentile), and the whiskers extend from the minimum to the maximum values. Statistical significance was defined as follows: *p ≤ 0.05, **p ≤ 0.01, ***p ≤ 0.001, ****p ≤ 0.0001.
Results
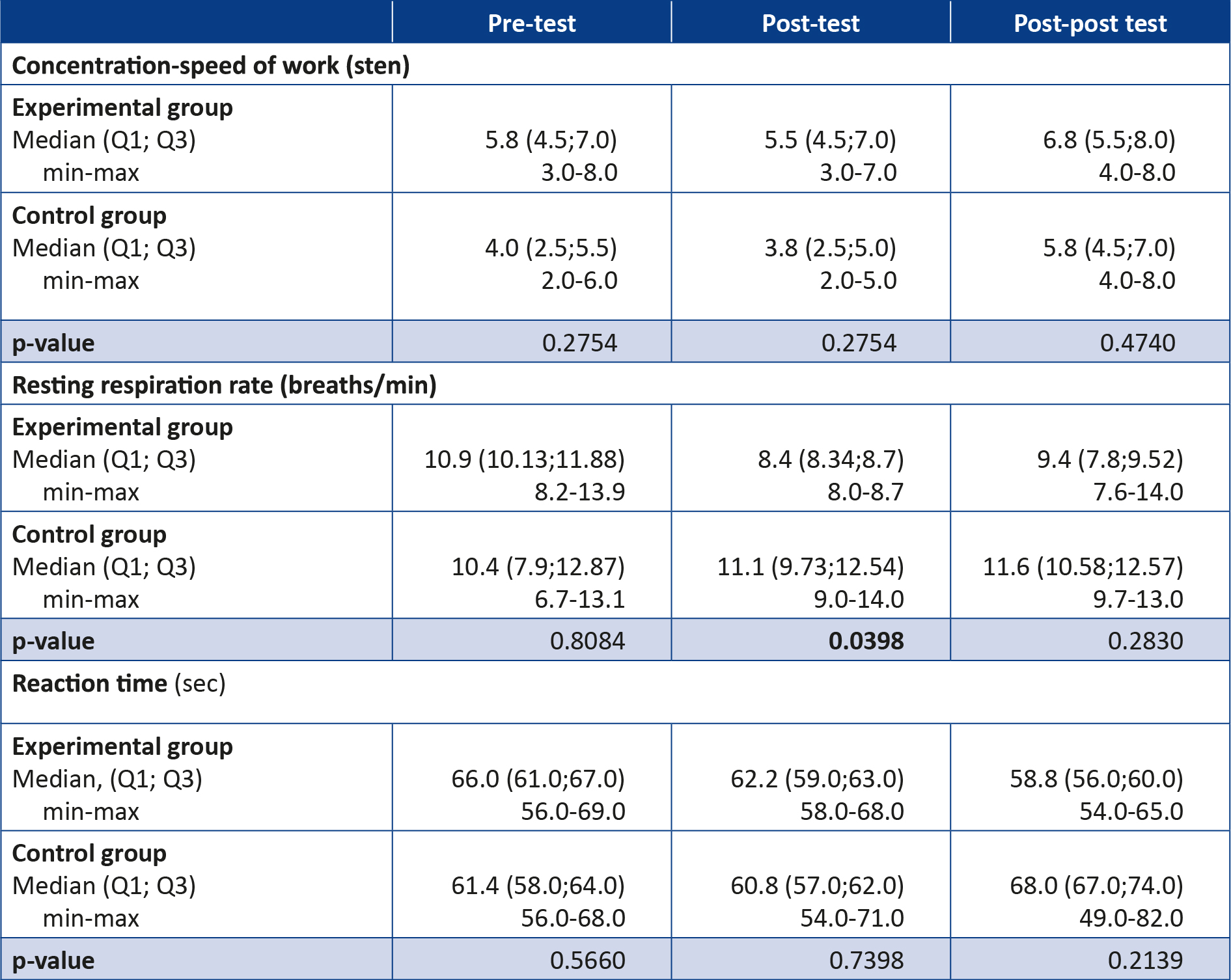
The descriptive statistical analysis conducted for concentration, resting respiratory rate and reaction time indicates a significant reduction in the frequency of resting breathing in athletes performing HRVB training (the average time for all from the experimental group was 807 min over the 4 weeks) compared to athletes not performing training; however, this trend was not maintained when athletes in the study group stopped performing regular HRVB training (Table 3).
Table 3. Statistical analysis with distribution of values for concentration (speed of work), resting respiration rate and reaction time
T-test, two-sided, homoscedastic
The remaining results indicated that the concentration and reaction time scores obtained in the respective tests did not differ significantly between the experimental and control groups.
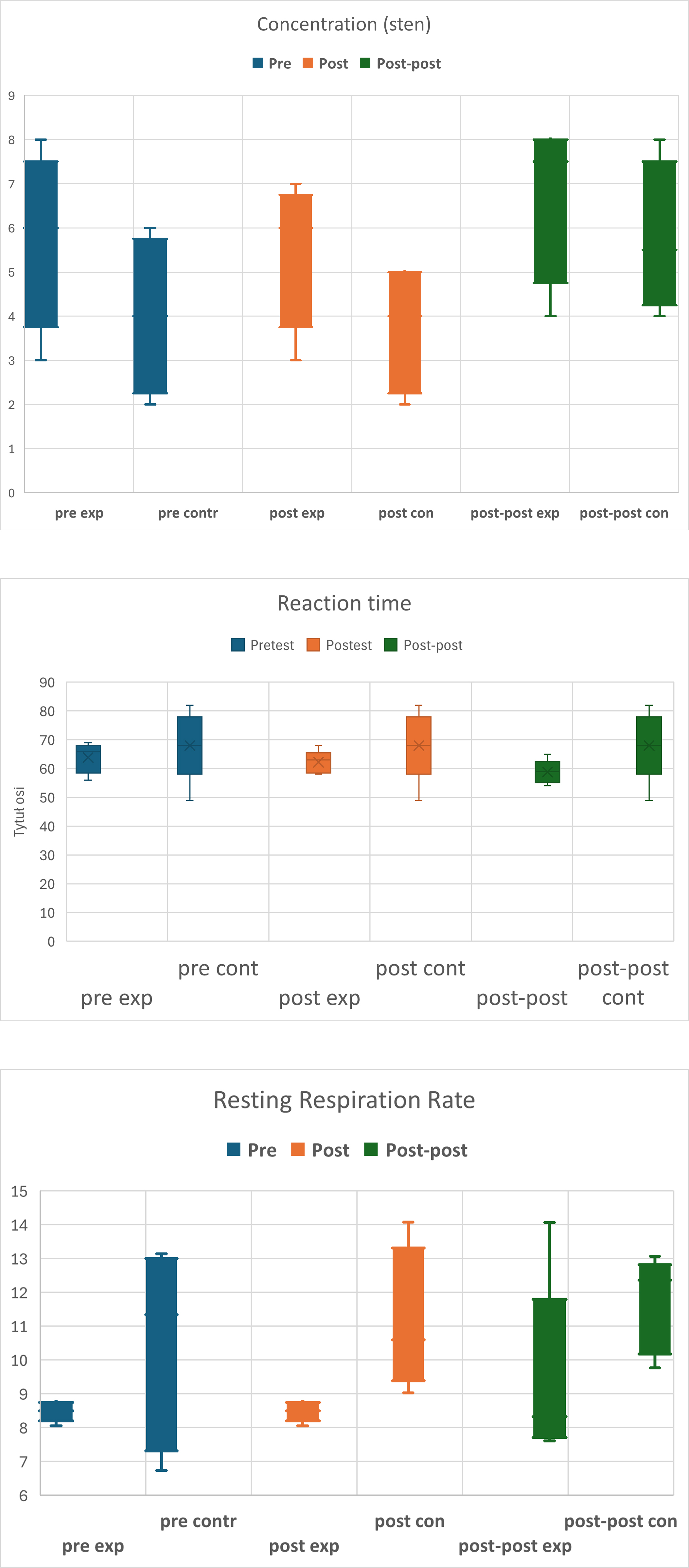
The analysis of the results at each stage indicates that reaction time in the experimental group improved over the course of the study, while in the control group, reaction time showed a slight improvement in the second measurement but significantly worsened in the final measurement. These results suggest that HRVB training can have a significant effect on improving reaction time in the experimental group in the final measurement (Figure 2).
Figure 2. Distribution of test scores in concentration, resting respiration rate, and reaction time across the respective measurement points
Statistically significant results: * p ≤ 0.05, ** p ≤ 0.01, *** p ≤ 0.001, **** p ≤ 0.0001; pre exp – pre-test experimental group, pre contr – pre-test control group, post exp – post-test experimental group, post contr – post-test control group, post-post exp – post-post test experimental group, post-post contr – post-post test control group
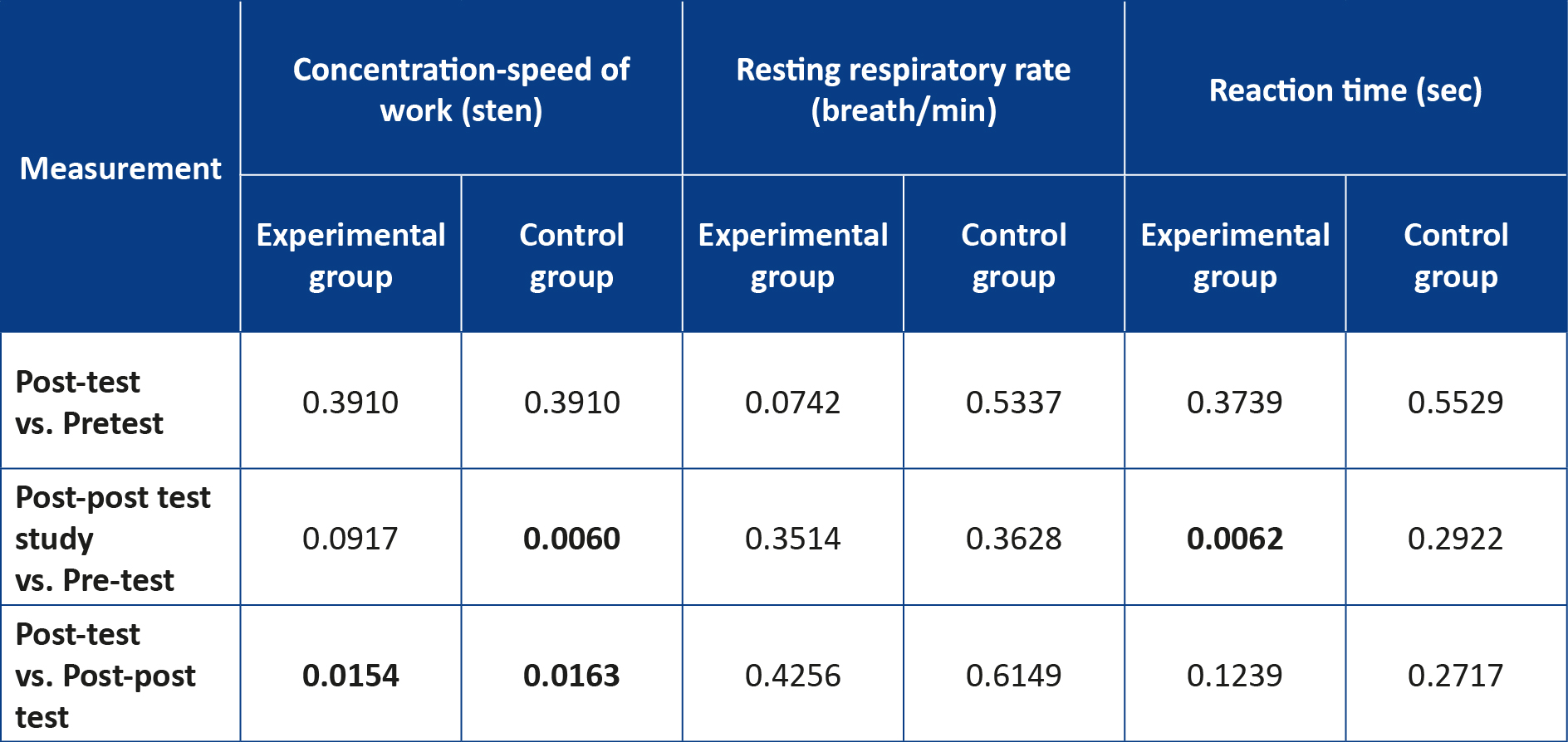
Furthermore, the analysis of concentration parameters, resting respiratory rate and reaction time within each group across measurement points revealed a statistically significant improvement in reaction time in the experimental group between the pre-test and post-post test measurements (Table 4).
Table 4. Statistical analysis between measurements for concentration (speed of work), resting respiratory rate and reaction time
T-test, two-sided, paired
In contrast, the same analysis indicated that the control group demonstrated a statistically significant improvement in concentration between the first and third measurements. Additionally, both groups showed substantial improvements in concentration between the second and third measurements. These findings may suggest that HRVB training did not have a significant impact on concentration among the athletes.
However, it is worth noting that the concentration scores in the experimental group were initially higher than those in the control group. Although the experimental group did not show improvement, the trend analysis indicates that it maintained a certain level of stability in performance. In contrast, the results from the control group showed considerable variability, meaning that athletes in this group occasionally achieved extremely high or extremely low scores in individual measurements. Given the small sample size, our results certainly require further investigation. The statistical analysis of changes in the resting respiratory rate did not reveal significant differences between the groups across the measurements.
HRV assessment
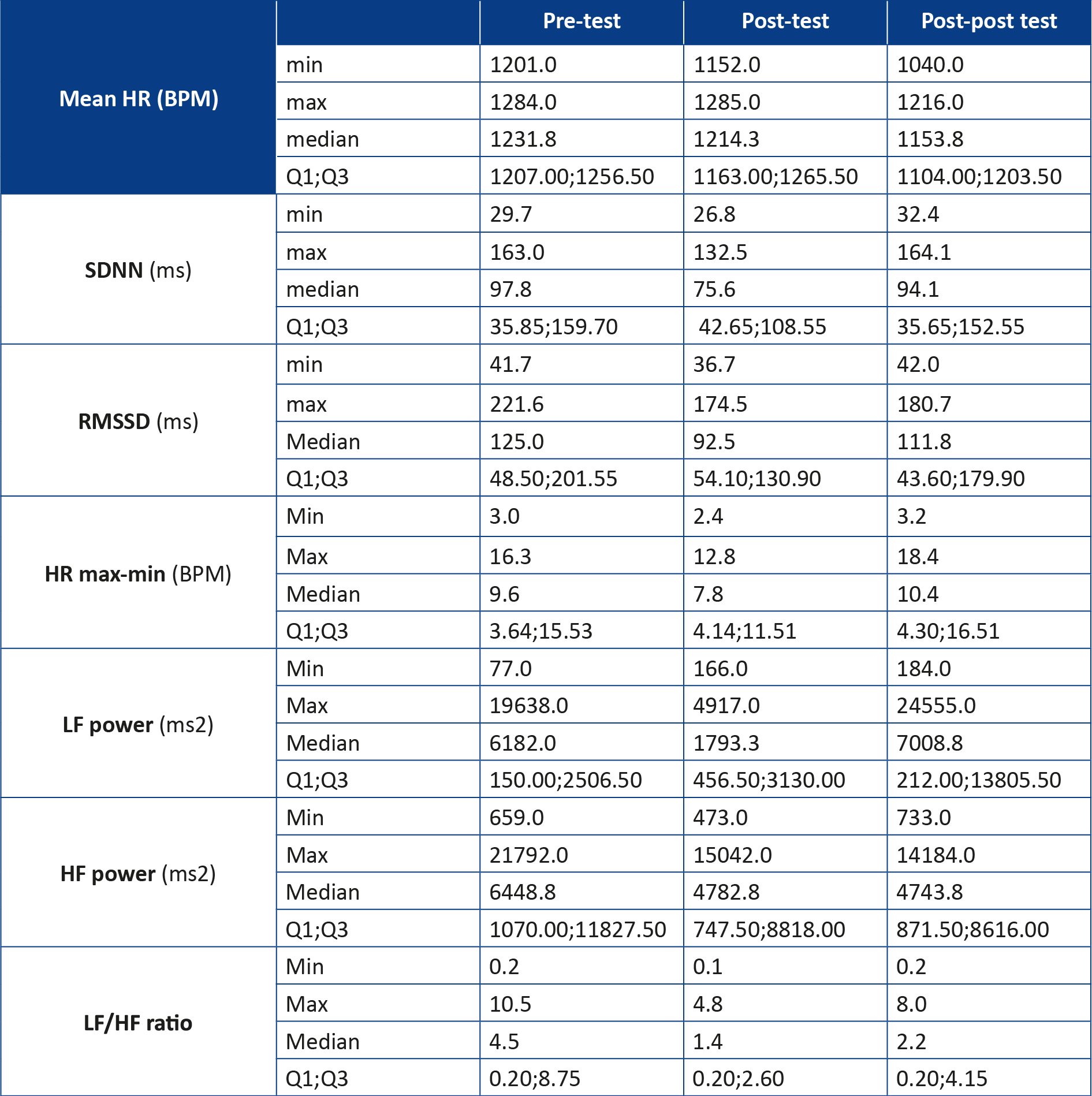
The results of the statistical analysis with the distribution of values of HRV (Table 5) and between the measurements for HRV (Table 6) for the study group indicate that there were no statistically significant differences. Due to the small sample size of the analyzed group, no analysis of the distributions of the values of the individual parameters was performed.
Table 5. Statistical analysis with distribution of values for heart rate variability in the experimental group
T-test, two-sided, paired. BPM – beats per minute; HF – high frequency; HR – heart rate; LF – low frequency; RMSSD – root mean square of successive RR interval differences; SDNN – standard deviation of RR intervals
Table 6. Statistical analysis between measurements for heart rate variability
P-values obtained via T-test, two-sided, paired. BPM – beats per minute; HF – high frequency; HR – heart rate; LF – low frequency; RMSSD – root mean square of successive RR interval differences; SDNN – standard deviation of RR intervals
Subjective stress
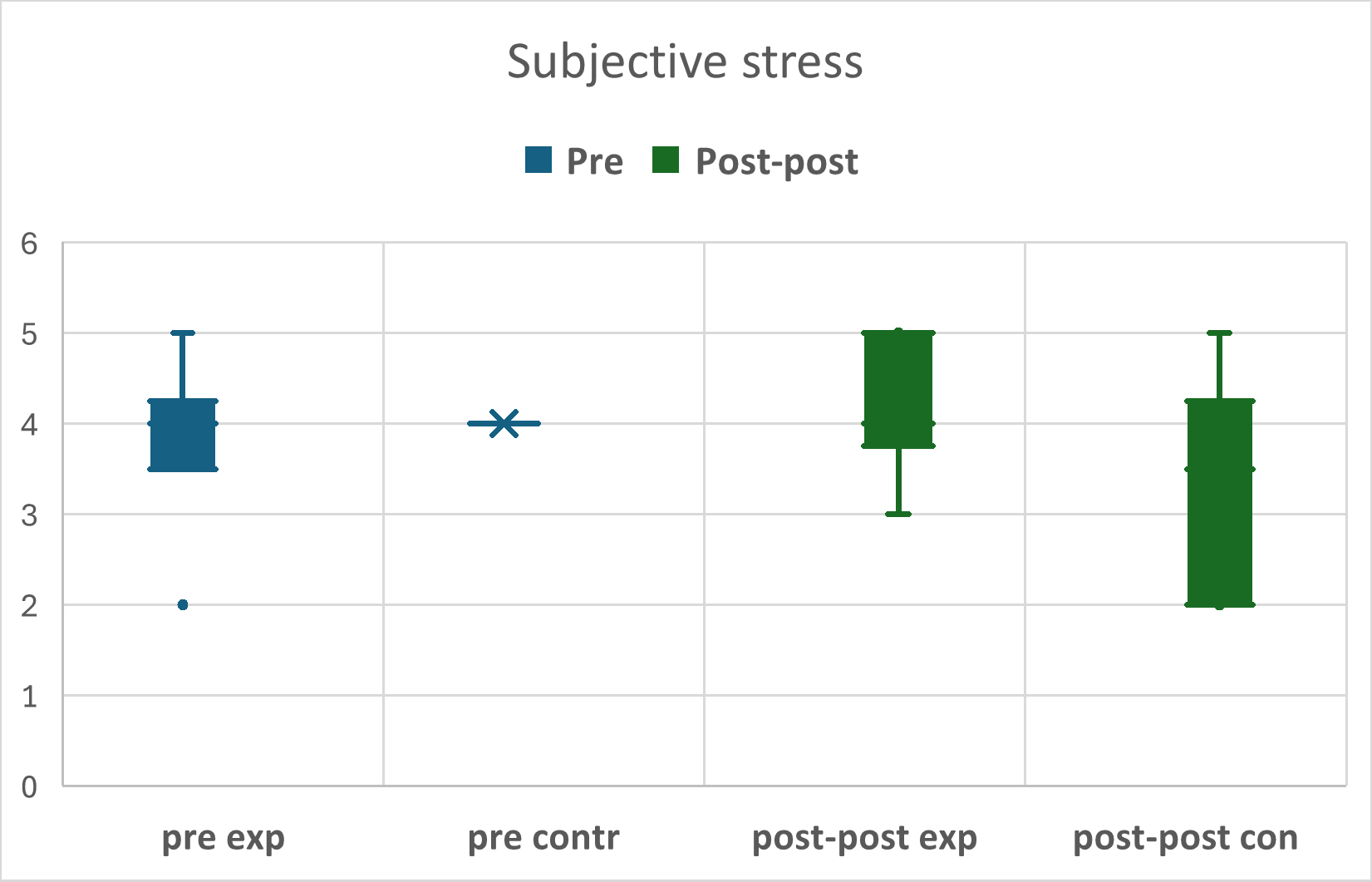
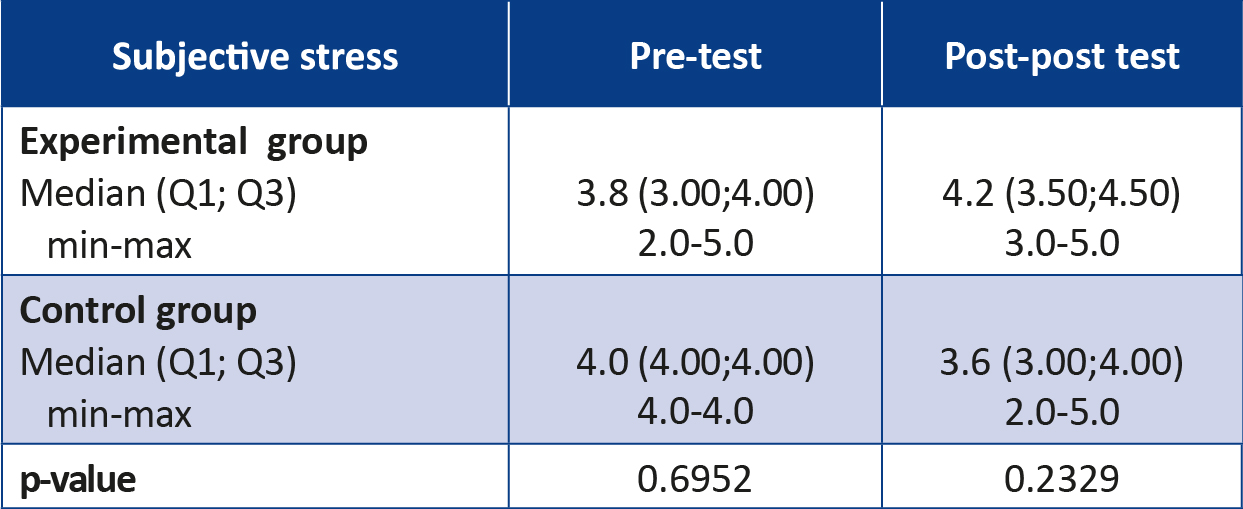
The statistical analysis of the parameter of the level of subjectively perceived stress shows that there were no statistically significant differences in subjective stress between the control and study groups, and both the control and study groups showed no significant statistical differences between the measurements of the two groups (Table 7). However, upon examining the distribution of individual results in both groups, it can be observed that the control group initially demonstrated greater stability, with athletes reporting a similar moderate level of perceived stress. In contrast, in the post-post test, the control group exhibited greater variability in reported stress levels compared to the experimental group (Figure 3).
Table 7. Subjective stress
T-test, two-sided, homoscedastic. 1 – high stress; 5 – low stress
Figure 3. Distribution of scores in the subjective stress test across the respective measure
pre exp – pre-test experimental group, pre contr – pre-test control group, post-post exp – post-post test experimental group, post-post contr – post-post test control group
Discussion
Our findings confirmed that HRVB training may improve the reaction time of rowers, consistent with previous research conducted among basketball players [17]. Improvement in reaction time is particularly relevant in a sport such as rowing, where the start is triggered by an auditory cue (a referee’s whistle), and may represent a critical component in professional and effective coaching strategies for athletes at this competitive level.
Additionally, our results indicate that HRVB training led to a significant reduction in resting respiratory rate within the experimental group. However, no statistically significant changes were observed in HRV parameters. Although changes in subjective stress levels did not reach statistical significance, a reduction in perceived stress was noted in the post-post test in the experimental group, whereas an increase was observed in the control group during the same measurement point.
Our findings may cautiously suggest that HRVB training, through its effects on respiratory regulation and pulmonary function, could contribute to autonomic nervous system modulation and stress reduction. This interpretation aligns with previous findings on the effectiveness of HRVB in managing conditions such as asthma, depression and anxiety in clinical psychology settings, as well as reducing anxiety in athletes [12, 14, 16, 20].
Given the highly demanding nature of elite-level rowing training and the observation that 5 out of 20 participants in this study scored high on the Beck Depression Inventory, it appears warranted to initiate a broader discussion around mental health in competitive sports. Introducing appropriate psychological support tools, including biofeedback-based interventions such as HRVB, may offer valuable assistance to athletes coping with the pressures of elite competition.
Interestingly, the concentration test results did not indicate a significant effect of HRVB training. However, the observed improvement in reaction time, which inherently requires a certain level of concentration, suggests a possible indirect influence. It may be beneficial in future studies to replace the current paper-and-pencil concentration test with a task more closely resembling competitive racing or decision-making under pressure, which may enhance the validity of the findings and increase the likelihood of detecting more consistent effects.
Limitations of the study
As this study represents the first of its kind conducted among Polish Olympic-level rowers, it is challenging for the authors to directly compare the results with those of previous research in this specific context. The pretests were carried out at the beginning of the athletes’ competition season and covered the typical course of the season, including participation in the most important competitions (e.g. European Championships or World Championships), ending with the post-post tests. This study, however, has certain limitations, such as the small sample size, the absence of a comprehensive HRV analysis, and a shortened intervention period (4 weeks instead of the 5 weeks recommended in the abbreviated Lehrer protocol). Despite promising results, including a reduction in reaction time by 0.18 seconds and a decrease in the resting respiratory rate, it is important to note that the small sample size, high degree of individualization in training, the psychophysiological variability among athletes suggest that coaches of other athletes should conduct preliminary testing before implementing this method during critical phases of the Olympic preparation period.
Future directions
Researching the effectiveness of using non-invasive and easy-to-apply methods to influence the psychophysical state of athletes is of vital importance in an era of increasingly high performance by athletes around the world. The identification of key psychophysical parameters for a particular sport, and the proper data collection must take place in cooperation with specialists from many fields. Only such research supported by knowledge from various fields of medical, sports or social sciences can bring researchers, coaches and athletes themselves closer to optimizing effective measures that result in winning medals in international competitions.
Conclusions
The results of our study suggest that HRVB training may reduce the resting respiratory rate in the experimental group and may improve the reaction time of athletes in accordance with applied methods in rowing.
This study was conducted as part of a research grant awarded by the Ministry of Sport and Tourism, in accordance with the terms specified in contract no. 2022/0768/0017/UDot/61/DSW.
Acknowledgements
The authors would like to thank those involved in this project from the Polish Federation of Rowing Associations, the Rehasport Clinic Sp. z o. o., and coaches Mariusz Goliński, Wojciech Jankowski and Piotr Buliński for their support in carrying out the project.
Conflict of interest
The authors declare that they have no conflict of interest.
Funding
None.
----------
Image credit: Faraz Khan; source – flickr.com (PDM 1.0)
References
| 1. |
Grgic J, Diaz-Lara FJ, Del Coso J, Duncan MJ, Tallis J, Pickering C, et al. The Effects of Caffeine Ingestion on Measures of Rowing Performance: A Systematic Review and Meta-Analysis. Nutrients [Internet]. 2020 Feb 8;12(2):434. Available from: https://www.mdpi.com/2072-6643/12/2/434.
|
| 2. |
Hwang W-S, Kim H-T. Changes in the Muscle Strength, Muscle Endurance, and Rowing Performance of University Rowing Athletes Following Kettlebell Training and Strength Training. Sport Sci [Internet]. 2024 Dec 31;42(3):27–35. Available from: https://kiss.kstudy.com/Detail/Ar?key=4151011.
|
| 3. |
Urbański R, Aschenbrenner P, Żmijewski P, Ewertowska P, Świtała K, Krzysztofik M. Effect of Simultaneous Lower- and Upper-Body Ischemic Preconditioning on Lactate, Heart Rate, and Rowing Performance in Healthy Males and Females. Appl Sci [Internet]. 2024 Apr 23;14(9):3539. Available from: https://www.mdpi.com/2076-3417/14/9/3539.
|
| 4. |
Latour E, Arlet J, Latour E, Latour M, Basta P, Skarpańska-Stejnborn A. Stressor-Induced Temporal Cortisol Deficiency as a Primary Trigger for Adaptation to Stress. Int J Environ Res Public Health [Internet]. 2022 May 5;19(9):5633. Available from: https://www.mdpi.com/1660-4601/19/9/5633.
|
| 5. |
Basta P, Skarpańska-Stejborn A, Pilaczyńska-Szcześniak Ł. Influence of Annual Training Cycle on Threshold Power and Reaction of Blood Antioxidative Stress Indices During A Standard Rowing Test. Hum Mov [Internet]. 2008 Jan 1;9(1) 41–45. Available from: https://pdfs.semanticscholar.org/5179/4d833a05f6824efff9f128623b66f28a271c.pdf
|
| 6. |
Kopeć A, Napierała M, Zukow W. Kontuzje i urazy w wioślarstwie= Injuries and trauma in rowing. J Educ Heal Sport [Internet]. 2016;6(4):331–54. Available from: https://apcz.umk.pl/JEHS/article/view/3484.
|
| 7. |
Heiss S, Vaschillo B, Vaschillo EG, Timko CA, Hormes JM. Heart rate variability as a biobehavioral marker of diverse psychopathologies: A review and argument for an “ideal range”. Neurosci Biobehav Rev [Internet]. 2021 Feb;121:144–55. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0149763420306795.
|
| 8. |
Fatisson J, Oswald V, Lalonde F. Influence Diagram of Physiological and Environmental Factors Affecting Heart Rate Variability: An Extended Literature Overview. Heart Int [Internet]. 2016 Jan 25;11(1):heartint.500023. Available from: http://journals.sagepub.com/doi/10.5301/heartint.5000232.
|
| 9. |
Aubert AE, Seps B, Beckers F. Heart Rate Variability in Athletes. Sport Med [Internet]. 2003;33(12):889–919. Available from: http://link.springer.com/10.2165/00007256-200333120-00003.
|
| 10. |
Staszak O. Odruch z baroreceptorów tętniczych w trakcie testu pochyleniowego u pacjentów z określonymi typami omdleń wazowagalnych. 2015.
|
| 11. |
Lehrer PM, Vaschillo E, Vaschillo B, Lu S-E, Eckberg DL, Edelberg R, et al. Heart Rate Variability Biofeedback Increases Baroreflex Gain and Peak Expiratory Flow. Psychosom Med [Internet]. 2003 Sep;65(5):796–805. Available from: https://journals.lww.com/00006842-200309000-00012.
|
| 12. |
Lehrer PM, Vaschillo E, Vaschillo B, Lu S-E, Scardella A, Siddique M, et al. Biofeedback Treatment for Asthma. Chest [Internet]. 2004 Aug;126(2):352–61. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0012369215311430.
|
| 13. |
Hallman DM, Olsson EMG, von Schéele B, Melin L, Lyskov E. Effects of Heart Rate Variability Biofeedback in Subjects with Stress-Related Chronic Neck Pain: A Pilot Study. Appl Psychophysiol Biofeedback [Internet]. 2011 Jun 2;36(2):71–80. Available from: http://link.springer.com/10.1007/s10484-011-9147-0.
|
| 14. |
Karavidas MK, Lehrer PM, Vaschillo E, Vaschillo B, Marin H, Buyske S, et al. Preliminary Results of an Open Label Study of Heart Rate Variability Biofeedback for the Treatment of Major Depression. Appl Psychophysiol Biofeedback [Internet]. 2007 Mar 26;32(1):19–30. Available from: http://link.springer.com/10.1007/s10484-006-9029-z.
|
| 15. |
Lin G, Xiang Q, Fu X, Wang S, Wang S, Chen S, et al. Heart Rate Variability Biofeedback Decreases Blood Pressure in Prehypertensive Subjects by Improving Autonomic Function and Baroreflex. J Altern Complement Med [Internet]. 2012 Feb;18(2):143–52. Available from: http://www.liebertpub.com/doi/10.1089/acm.2010.0607.
|
| 16. |
Goessl VC, Curtiss JE, Hofmann SG. The effect of heart rate variability biofeedback training on stress and anxiety: a meta-analysis. Psychol Med [Internet]. 2017 Nov 8;47(15):2578–86. Available from: https://www.cambridge.org/core/product/identifier/S0033291717001003/type/journal_article.
|
| 17. |
Paul M, Garg K, Singh Sandhu J. Role of Biofeedback in Optimizing Psychomotor Performance in Sports. Asian J Sports Med [Internet]. 2012 Mar 1;3(1). Available from: https://brieflands.com/articles/asjsm-76716.html.
|
| 18. |
Deschodt-Arsac V, Lalanne R, Spiluttini B, Bertin C, Arsac LM. Effects of heart rate variability biofeedback training in athletes exposed to stress of university examinations. Subramanian SK, editor. PLoS One [Internet]. 2018 Jul 26;13(7):e0201388. Available from: https://dx.plos.org/10.1371/journal.pone.0201388.
|
| 19. |
Mueller K, Williams PS, Haley L, Heick J. Heart Rate Variability Biofeedback Improves Sports Performance in an Elite Female Athlete. Cardiopulm Phys Ther J [Internet]. 2020 Jul;31(3):123–32. Available from: https://journals.lww.com/10.1097/CPT.0000000000000120.
|
| 20. |
Lagos L, Vaschillo E, Vaschillo B, Lehrer P, Bates M, Pandina R. Virtual reality–assisted heart rate variability biofeedback as a strategy to improve golf performance: a case study. Biofeedback [Internet]. 2011;39(1):15–20. Available from: https://meridian.allenpress.com/biofeedback/article-abstract/39/1/15/113152.
|
| 21. |
Choudhary R, Trivedi V, Choudhary S. EFFECT OF HEART RATE VARIABILITY BIOFEEDBACK TRAINING ON THE PERFORMANCE OF TRACK ATHLETE. Int J Ther Rehabil Res [Internet]. 2016;5(4):166. Available from: http://www.scopemed.org/fulltextpdf.php?mno=220490.
|
| 22. |
Jiménez Morgan S, Molina Mora JA. Effect of Heart Rate Variability Biofeedback on Sport Performance, a Systematic Review. Appl Psychophysiol Biofeedback [Internet]. 2017 Sep 1;42(3):235–45. Available from: http://link.springer.com/10.1007/s10484-017-9364-2.
|
| 23. |
Beck AT, Steer RA, Brown GK. BDI®-II [in Polish]. 2nd ed. Pracownia Testów Psychologicznych Polskiego Towarzystwa Psychologicznego; 2019.
|
| 24. |
Ciechanowicz A, Stańczak J. TUS. Testy Uwagi i Spostrzegawczości. Wersja 6/9 – normy dla dorosłych [in Polish]. Pracownia Testów Psychologicznych Polskiego Towarzystwa Psychologicznego; 2006.
|
| 25. |
Lehrer P, Vaschillo B, Zucker T, Graves J, Katsamanis M, Aviles M, et al. Protocol for Heart Rate Variability Biofeedback Training. Biofeedback [Internet]. 2013;41(3):98–109. Available from: https://biofeedback.kglmeridian.com/view/journals/biof/41/3/article-p98.xml.
|
