


Unusual acute idiopathic scrotal edema – could it be a separate disease (chronic idiopathic scrotal edema)?


Abstract
Acute idiopathic scrotal edema (AISE) is a rare, mild and self-limiting disease. The etiology and pathogenesis of this disease remain unclear. Diagnosing AISE requires the exclusion of other scrotal disorders. We report a 48-year-old Caucasian male patient admitted to the Department of Urology with an atypical course of AISE which persisted for 12 months, despite adequate conservative treatment. Accordingly, we propose a new term, chronic idiopathic scrotal edema (CISE), to describe an extremely rare cause of bilateral scrotal edema in adults.
Citation
Czajkowski M, Gibas A, Czajkowska K, Dolny M, Sokołowska-Wojdyło M, Matuszewski M. Unusual acute idiopathic scrotal edema – could it be a separate disease (chronic idiopathic scrotal edema)?. Eur J Transl Clin Med. 2024;7(2):22-25





Introduction
Acute idiopathic scrotal edema (AISE) is a rare, mild and self-limiting disease. Its etiology and pathogenesis are unknown. AISE is mainly found in young boys but can also occur in adult men [1-2]. Determining the diagnosis of AISE requires the exclusion of other scrotal disorders (Table 1). The onset of AISE is sudden, but the symptoms usually resolve spontaneously within 3-5 days. Unilateral enlargement of the scrotum is observed in more than half of cases [1]. Patients most often complain of pain in the scrotum and erythema of the groin [1]. Ultrasound examination reveals a swollen and thickened scrotal wall without involvement of the deeper layer structures (testis or epididymis). Hypervascularity of the scrotum (fountain sign visible in the horizontal plane) is a common symptom [2]. We present a case of an atypical course of AISE which persisted for one year, despite adequate conservative treatment. Due to the long duration the disease, we decided to treat surgically. During 5 years of follow-up, the symptoms of idiopathic scrotal edema have not recurred. Our aim was to describe an atypical course of a long-lasting idiopathic scrotal edema in an adult and to present surgery as an effective method of treatment.
Case report
A 48-year-old Caucasian male was admitted to the Department of Urology with the chief complaint of massive edema of the scrotum accompanied by pain, erythema and discomfort (Figure 1]. The symptoms began 12 months ago, resulting in loss of sexual activity due to penis buried in the edema and erectile dysfunction (15 points on the IIEF-5 (International Index of Erectile Function) questionnaire). The patient denied having allergies, previous surgeries (i.e. penile enlargement procedures) or scrotal trauma. His current medical history included hypertension, gout, obesity (BMI = 37 kg/m²) and he was an active tobacco smoker with a 20 pack-year history). He took a variety of medications, including alpha blockers, beta blockers, calcium blockers, diuretics and sartans. The patient stated that the edema of the scrotum occurred 12 months earlier and since then has led to lower quality of life, particularly in terms of social interaction.
Figure 1. Massive edema of the scrotum in the course of the chronic idiopathic scrotal edema
The patient’s scrotum was significantly enlarged, with smooth, painful skin on palpation. His penis was engulfed by the swollen scrotum. The inguinal nodes were not enlarged.
Colonoscopy and computed tomography of the abdomen and pelvis were performed and did not reveal any cause of the edema was found. Ultrasonography of the scrotum revealed a positive fountain sign and scrotal wall thickness of approximately 4 cm.
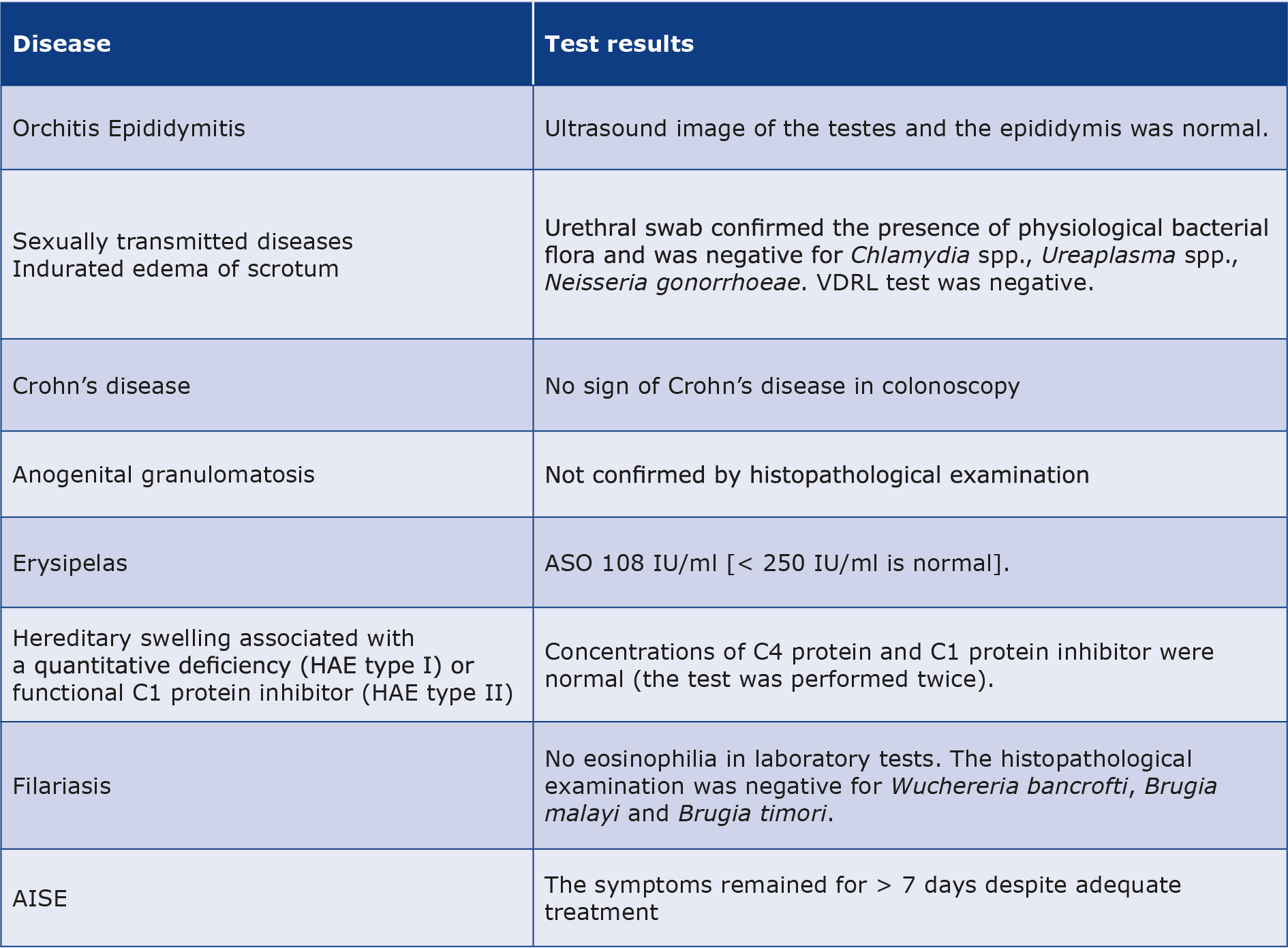
Due to the unclear etiology of this long-lasting scrotal edema, an in-depth differential diagnosis was performed (Table 1). Microscopic examination of the incisional skin biopsy specimen taken from the scrotal wall revealed nonspecific inflammatory lesions. There was no improvement after 1 month of treatment with non-steroidal anti-inflammatory drugs (NSAIDs), antibiotics, antihistamines and also after changing some of the medications the patient was taking in chronically. Therefore, other causes of scrotal edema were excluded.
Table 1. The differential diagnosis for chronic idiopathic scrotal edema
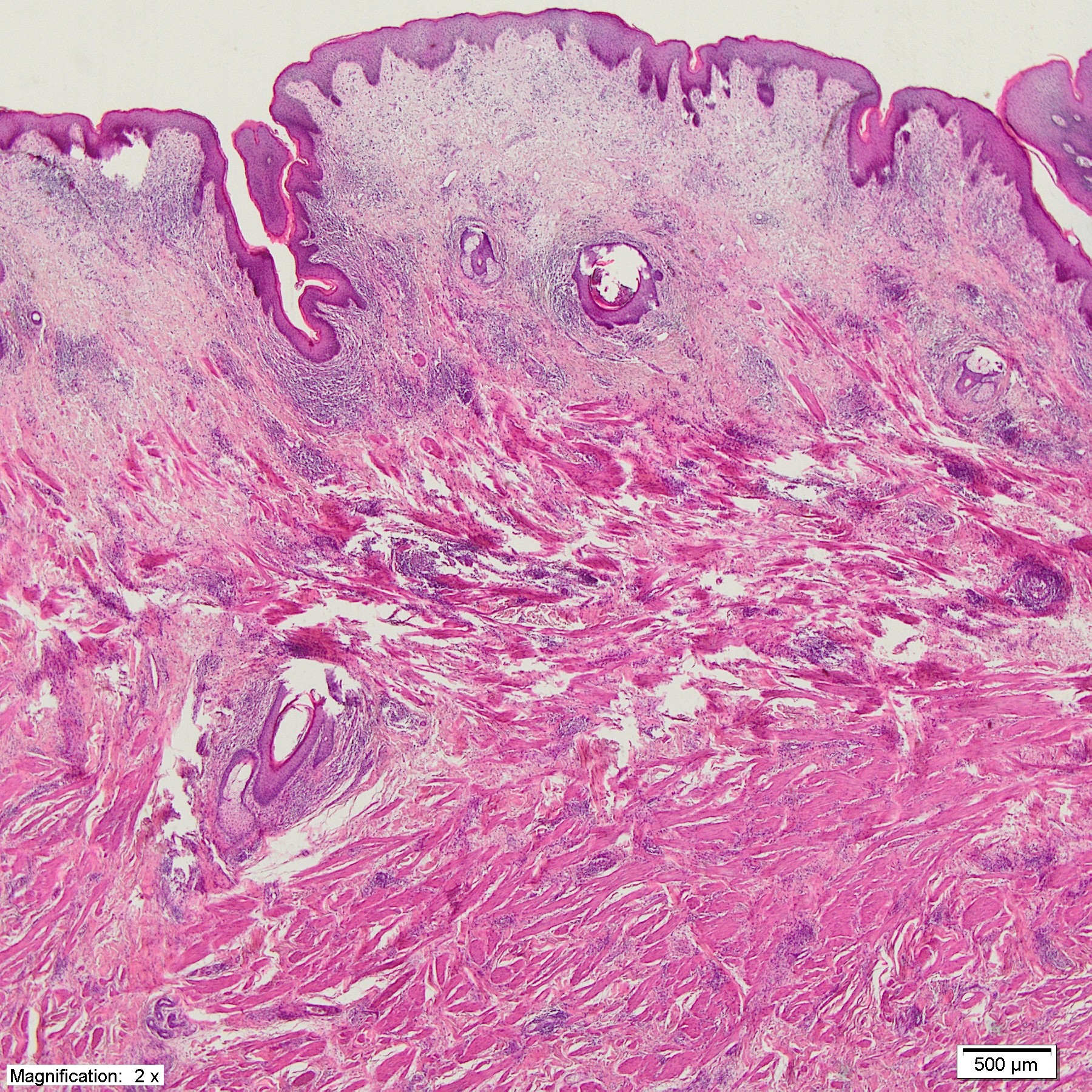
Due to the scrotal edema and the reported discomfort, it was decided to perform scrotal surgery. The scrotum was resected and the testes were placed in the perineum. Microscopic analysis of all the collected samples revealed nonspecific inflammatory lesions in the skin and subcutaneous tissue (Figure 2). In five-years follow-up no further scrotum edema, pain or erythema was observed (Figure 3). The patient reported being sexually active with good erectile function (IIEF-5 score 23 points) and denied any problems related to testicular placement in the perineum.
Figure 2. The histopathological examination revealed numerous, dilated lymphatic vessels, fibrosis within the dermis and foci of chronic inflammatory infiltration
Figure 3. Outpatient follow-up
Discussion
Diagnosis of AISE requires the exclusion of other scrotal disorders [1, 3-5]. As shown in Table 1, none of these tests indicated an unequivocal cause of our patient’s scrotal edema. However, scrotal ultrasound examination has revealed the “fountain sign,” which was first described by Geiger as highly suggestive of the diagnosis of AISE [2-3]. Other possible ultrasound findings in AISE include reactive hydrocele and enlargement of inguinal nodes [3].
Sudden onset and spontaneous regression of scrotal edema within 3-5 days is typical for AISE. Conservative treatment including bed rest and activity restriction, NSAIDs, antibiotics and antihistamines have been established as the treatment of choice [1, 3-5]. As stated by Santi et al., there are no cases of AISE with duration of more than 7 days [1]. In all cases of AISE reported to date, surgical treatment was described as the wrong choice [1, 3-5]. However, we would like to ask the question: what should be the next step when the scrotal edema persists despite adequate conservative treatment?
Conclusions
Based on the case described above, we suggest a new term, Chronic Idiopathic Scrotal Edema (CISE), to describe an extremely rare cause of bilateral scrotal edema in adults.
The main differences between acute and chronic scrotal edema (AISE vs. CISE) are the duration of the disease (< 7 days vs. ≥ 7 days) and the method of treatment (conservative vs. surgery). Further studies are needed to confirm our findings.
Statement of ethics
The patient provided written informed consent to publish this case report.
Conflict of interest
The authors declare that they have no conflicts of interest.
Funding
Not applicable.
References
| 1. |
Santi M, Lava S, Simonetti G, Bianchetti M, Milani G. Acute Idiopathic Scrotal Edema: Systematic Literature Review. Eur J Pediatr Surg [Internet]. 2018;28(03):222–6. Available from: http://www.thieme-connect.de/DOI/DOI?10.1055/s-0037-1603089.
|
| 2. |
Geiger J, Epelman M, Darge K. The Fountain Sign. J Ultrasound Med [Internet]. 2010 (8):1233–7. Available from: http://doi.wiley.com/10.7863/jum.2010.29.8.1233.
|
| 3. |
Lee A, Park SJ, Lee HK, Hong HS, Lee BH, Kim DH. Acute idiopathic scrotal edema: ultrasonographic findings at an emergency unit. Eur Radiol [Internet]. 2009;19(8):2075–80. Available from: http://link.springer.com/10.1007/s00330-009-1356-z.
|
| 4. |
Breen M, Murphy K, Chow J, Kiely E, O’Regan K. Acute Idiopathic Scrotal Edema. Case Rep Urol [Internet]. 2013;2013:1–3. Available from: http://www.hindawi.com/journals/criu/2013/829345/.
|
| 5. |
Braun MM, Cronin AJ, Bell DG. A Case Report of Acute Idiopathic Scrotal Edema. Mil Med [Internet]. 2013;178(7):e890–2. Available from: https://academic.oup.com/milmed/article/178/7/e890-e892/4243592.
|
