


ST segment depression in atrioventricular reentrant tachycardia


Abstract
Background: ST segment deviation is common in patients with narrow QRS complex tachycardia. It mainly concerns young people in whom ischemic background is unlikely. In our work we would also like to propose another potential mechanism – the overlapping of individual components of the QRS complex.
Material and methods: The study included 11 patients (7 women and 4 men) with paroxysmal narrow QRS complex tachycardia. An electrophysiological study was performed in all patients, the diagnosis of atrioventricular reentrant tachycardia was established and finally successful RF ablation was done. We measured the individual components of QRS QR, RS and RJ during sinus rhythm and during tachycardia.
Results: The difference RJ-QR during tachycardia correlated negatively with tachycardia cycle length T(r = -0.85, p = 0.000831 ). We also showed a significant difference between the amplitude of the RJ segment in tachycardia and during sinus rhythm (p = 0.005), at the same time we showed no differences between the amplitude of QR and RS.
Conclusions: We showed a statistically significant difference in ST segment depression in correlation with the rate of tachycardia in patients with AVRT resulting mainly from the overlapping of individual components of the QRS complex.
Citation
Mercik J S, Kuniewicz M, Radziejewska J, Pach K, Zyśko D, Gajek J. ST segment depression in atrioventricular reentrant tachycardia. Eur J Transl Clin Med. 2023;6(2):66-70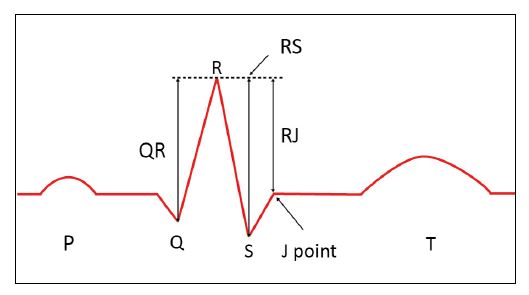






Abbreviations
- AV – atrioventricular
- AVNRT – atrioventricular nodal reentry tachycardia
- AVRT – atrioventricular reentrant tachycardia
- ECG – electrocardiogram
- EPS – electrophysiological study
Introduction
ST segment changes are mainly associated with coronary artery disease (CAD). However, in supraventricular tachycardias (SVTs) ST segment changes are common and may affect to 50-60% of patients with atrioventricular nodal reentry tachycardia (AVNRT) and atrioventricular reentrant tachycardia (AVRT) [1]. In patients with AVNRT or AVRT, the change in the ST segment on the electrocardiogram (ECG) most often takes the form of downward oblique deviation [2]. Vast majority of these patients are healthy, young people in whom cardiac ischemia is unlikely [3]. The ST segment changes during episodes of SVT has been discussed many times, but none of these studies demonstrated a clear mechanism responsible for the ST segment deviations [4-5]. In this paper, we discuss the potential explanation of ST segment changes in AVRT. We also propose another potential mechanism – the overlapping of individual components of the QRS-T complex resulting in a change in the baseline reference point and a measurement artifact in the form of ST segment depression.
Materials and methods
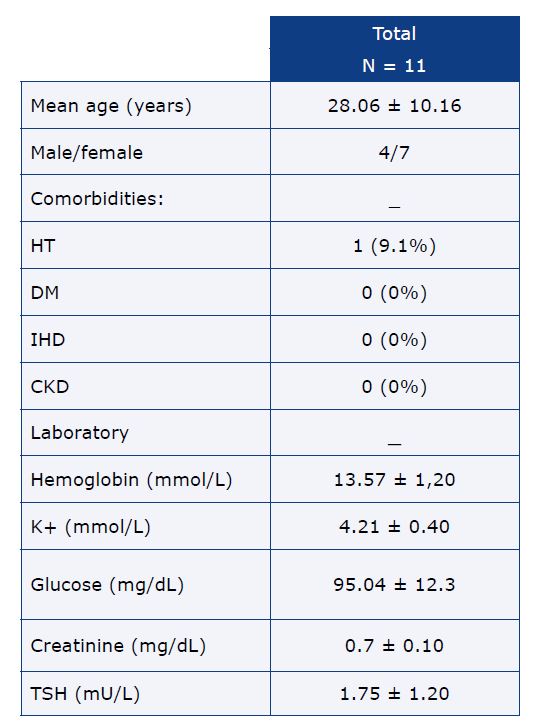
11 patients (7 women and 4 men) took part in the study, their average age was about 28 years. All patients underwent an electrophysiological study (EPS), during which the diagnosis of AVRT was made, followed by successful radiofrequency ablation of the accessory pathway was performed. Detailed demographic, clinical, and laboratory data are described in Table 1.
Table 1. Clinical characteristics of studied patients
HT – arterial hypertension, DM – diabetes mellitus, CKD – chronic kidney disease, IHD – ischemic heart disease, HF – heart failure
We assessed the ECG analogously to our earlier work on AVNRT [6-7]. Figure 1 shows how the individual components of the QRS complex were measured. Due to the best visibility of the R wave, lead V5 was used for all measurements.
Figure 1. Individual components of the QRS complex
QR segment – the distance between the bottom of the Q wave and the peak of the R wave, RS segment – the distance between the peak of the R wave and the bottom of the S wave, RJ segment – the segment between the peak of the R wave and the J point
The statistical analysis was performed using the computer program Statistica v. 13.3 (StatSoft Inc., Tulsa, USA). The Shapiro-Wilk W test was used to calculate normality of distribution, we used the Wilcoxon test for dependent groups for comparisons, and the Spearman’s test for correlation. The study was approved by the local Bioethical Committee at Wroclaw Medical University number KB – 213/2020.
Results
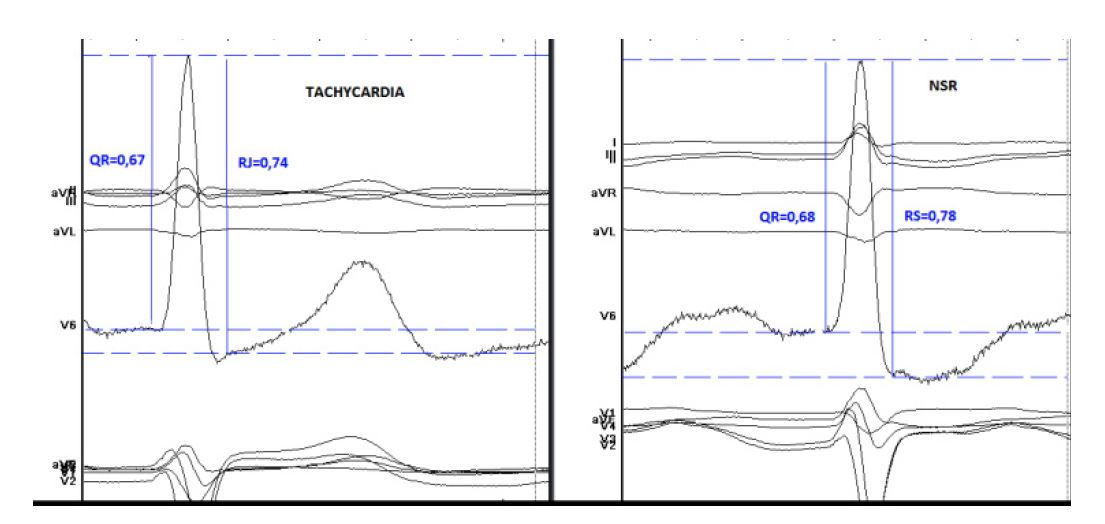
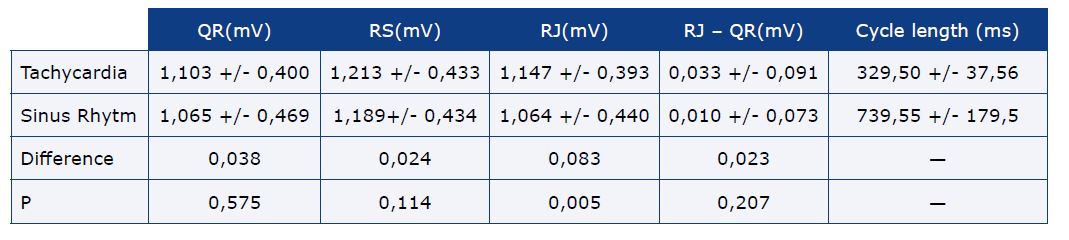
ECG parameters are presented in Table 2 and Figure 2. We noted a significant difference between the amplitude of the RJ segment in tachycardia and during sinus rhythm (p = 0.005). At the same time we found no differences between the amplitude of QR and RS.
Figure 2. QR and RJ measurements during tachycardia (left panel) and during sinus rhythm (right panel)
NSR – normal sinus rhythm
Table 2. The basic electrocardiographic parameters measurements in sinus rhythm and tachycardia with according differences and statistical
test results
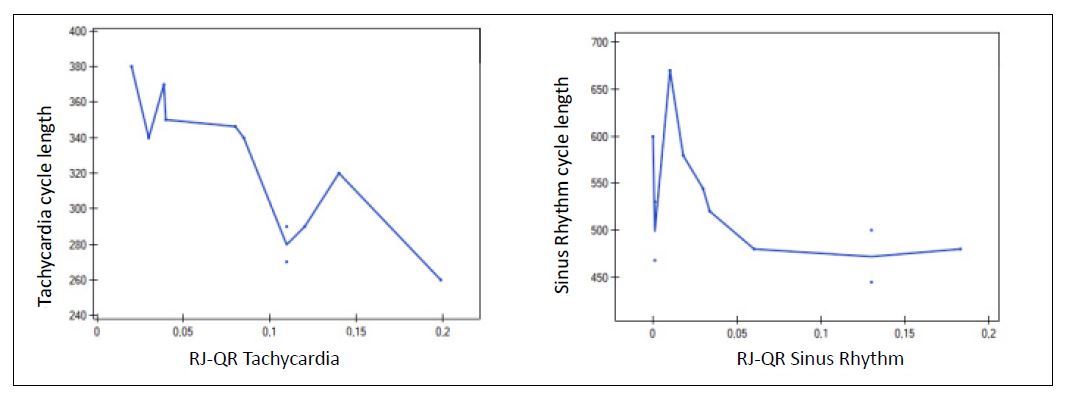
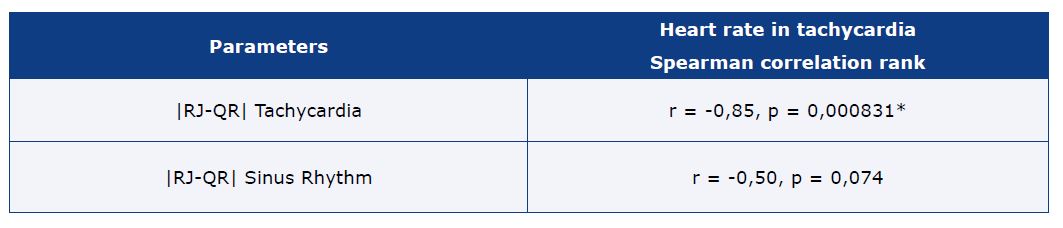
We also showed a significant negative correlation between the tachycardia cycle length and the RJ-QR difference – the faster the arrhythmia, the greater the ST segment denivelation (r = -0.85, p = 0.000831). During sinus rhythm, there were no significant changes in RJ-QR difference.
A graphical representation of the above-mentioned relationships is shown in Figure 3.
Figure 3. A graphical representation of the above-mentioned dependencies: RJ-QR (mV) during tachycardia (ms) (left panel) and during sinus rhythm (ms) (right panel)
In the graph on the left there is a strong dependence of RJ-QR on tachycardia, while during sinus rhythm (graph on the right) this relationship is not statistically significant (although its values are close to the level of statistical significance).
Table 3. The correlation of RJ-QR in tachycardia and sinus rhythm with tachycardia cycle length
Discussion
In patients with AVRT, there is a phenomenon of ST segment depression. Because this tachycardia affects mainly young people in whom ischemic etiology is unlikely, the most probable cause is a measurement artefact – the overlapping of individual components of the QRS complex and elevation of the baseline, a retrograde P wave or QRS alternans [1].
ST segment depression during SVT is well-documented in the literature [4-5]. These changes usually resolve when sinus rhythm is restored, although it has been reported that ST-segment depression may persist and is not associated with CAD-related myocardial damage [3].
Dorenkamp et al. concluded that there is no correlation between the presence of CAD and ST segment depression in ECG of patients with paroxysmal SVT [1]. The same percentage of people with ST segment depression was observed both among patients with significant narrowing in the coronary vessels and in patients with normal coronary angiography results.
In our study, we demonstrated a positive correlation between ST segment depression and arrhythmia rate. The shorter the arrhythmia cycle, the greater the overlap of the T wave of the previous QRS complex with the next QRS complex, which causes a rise the baseline and may give the impression of ST segment depression. We proposed a similar explanation for the AVNRT in another article [6].
During fast AVRT, in some patients there is an QRS alternans. Due to the dynamic change in the amplitude of all components of the QRS complex (QR, RS, RJ) from beat to beat, there is a change in the baseline, which may look like a depression of the ST segment. The QRS alternans in AVRT has not been explained, some studies suggest intraventricular conduction disturbances as the cause of this phenomenon [6]. In our study, unfortunately, we did not have patients with QRS alternans during orthodromic tachycardia.
A retrograde P wave occurs during AVRT. In orthodromic AVRT, the interval between the QRS complex and the retrograde P wave should be at least 70 ms, depending on the electrophysiological properties of the accessory pathway and the location between pathway and AV node [7]. For this reason, the retrograde P wave is projected onto the ST segment or the T wave. This may cause ST segment depression, which looks like its denivelations, likewise to myocardial ischemia. Riviera et al reached similar conclusions [8].
When considering the spatiotemporal relationships of retrograde atrial activation during AVRT, the possible locations of accessory pathways should be considered [9]. Viewed from the V5 lead, the left-sided accessory pathways generate retrograde P waves that will be negative, inducing a lowering of the J point and ST-segment in this lead. Right lateral pathways cause opposite changes inducing the relative elevation of the J point and the ST segment of the electrocardiogram in lead V5. Septal tracts induce similar changes, as activation of the left atrium electrically prevails over activation of the right atrium, but in this location the retrograde P wave is exceptionally short, which means that, depending on the speed of retrograde conduction, the change in a targeted manner may influence the J point or a fragment of the ST segment. Posterior pathways, depending on the location, can affect the described phenomenon in different ways. Therefore, in the case of our results, obtained in a relatively small study group, the relationships described do not have to be unambiguous. A probabilistic conclusion may be that the relationship described earlier is true, modified only by the influence of the retrograde P wave depending on the location of the accessory pathway [10-11].
Limitations
This is a single-center study conducted in a small group of patients. Because AVRT is a rare arrhythmia, there are significant difficulties in gathering a larger group of patients. None of the patients had coronary angiography performed to completely exclude the ischemic cause of ST segment changes. In addition, there was no exercise test performed and no pacing with the arrhythmia rate during the EPS to reproduce the baseline conditions during arrhythmia.
Conclusions
The cause of ST-T segment changes during AVRT remains unexplained. In this paper we propose a fairly simple but important explanation. The concept of ST segment change as a measurement artifact resulting from the overlapping of individual components of the QRS-T complex in AVRT has not been described in the literature so far. More research is needed to confirm this concept and to search for other potential mechanisms.
Conflicts of interest
None to report.
Funding
Not applicable.
References
| 1. |
Dorenkamp M, Zabel M, Sticherling C. Role of coronary angiography before radiofrequency ablation in patients presenting with paroxysmal supraventricular tachycardia. J Cardiovasc Pharmacol Ther [Internet]. 2007;12(2):137-44. Available from: https://doi.org/10.1177/10742484073007752.
|
| 2. |
Habash F, Albashaireh A, Madmani ME, Paydak H. ST segment elevation and depressions in supraventricular tachycardia without coronary artery disease. Rodriguez AE, editor. Case Reports Cardiol [Internet]. 2018:2716312. Available from: https://doi.org/10.1155/2018/2716312.
|
| 3. |
Elikowski W, Baszko A, Wróblewski D, Słomczyński M, Małek M. [Supraventricular tachycardia as a cause of elevated troponin I in a patient with normal coronary arteries]. Pol Merkur Lekarski [Internet]. 2005;18(108):696-9. Available from: http://www.ncbi.nlm.nih.gov/pubmed/16124386.
|
| 4. |
Nelson SD, Kou WH, Annesley T, de Buitleir M, Morady F. Significance of ST segment depression during paroxysmal supraventricular tachycardia. J Am Coll Cardiol [Internet]. 1988;12(2):383-7. Available from: http://www.ncbi.nlm.nih.gov/pubmed/3392331.
|
| 5. |
Habash F, Albashaireh A, Madmani ME, Paydak H. ST segment elevation and depressions in supraventricular tachycardia without coronary artery disease. Case reports Cardiol [Internet]. 2018:2716312. Available from: http://www.ncbi.nlm.nih.gov/pubmed/30647973.
|
| 6. |
Mercik J, Radziejewska J, Pach K, Zawadzki G, Zyśko D, Gajek J. ST-segment depression in atrioventricular nodal reentrant tachycardia: Important finding or just an artifact? Medicine (Baltimore) [Internet]. 2022;101(49):e31806. Available from: https://journals.lww.com/10.1097/MD.0000000000031806.
|
| 7. |
Mercik J, Radziejewska J, Pach K, Zyśko D, Gajek J. ST-segment depression in atrioventricular nodal reentrant tachycardia: Preliminary results. Adv Clin Exp Med [Internet]. 2021;30(12):1323-8. Available from: https://advances.umw.edu.pl/en/article/2021/30/12/1323/.
|
| 8. |
Roten L, Delacrétaz E. QRS alternans and cycle length oscillation during narrow QRS tachycardia. EP Eur [Internet]. 2008;10(6):778. Available from: https://doi.org/10.1093/europace/eun116.
|
| 9. |
Obel OA, Camm AJ. Accessory pathway reciprocating tachycardia. Eur Heart J [Internet]. 1998;19 Suppl E:E13-24, E50-1. Available from: http://www.ncbi.nlm.nih.gov/pubmed/9717020.
|
| 10. |
Rivera S, Paz Ricapito MD LA, Conde D, Verdu MB, Roux JF, Paredes FA. The retrograde p-wave theory: explaining ST segment depression in supraventricular tachycardia by retrograde AV node conduction. Pacing Clin Electrophysiol [Internet]. 2014;37(9):1100-5. Available from: https://onlinelibrary.wiley.com/doi/10.1111/pace.12394.
|
| 11. |
Ching-Tai T, Shih-Ann C, Chern-En C, Shih-Huang L, Zu-Chi W, Chuen-Wang C, et al. A new electrocardiographic algorithm using retrograde p waves for differentiating atrioventricular node reentrant tachycardia from atrioventricular reciprocating tachycardia mediated by concealed accessory pathway. J Am Coll Cardiol [Internet]. 1997;29(2):394-402. Available from https://doi.org/10.1016/S0735-1097(96)00490-1.
|
