


Usage of pregabalin in the treatment of pain associated with chronic pancreatitis – a clinically oriented narrative review


Abstract
Abdominal pain is one of the main symptoms of pancreatic diseases, including chronic pancreatitis (CP). Once the disease is in remission, pain management is a key element of treatment. Co-analgesics may also be used at any stage of analgesia, among which antiepileptic drugs such as pregabalin. The first data on the beneficial effect of pregabalin on pain in the course of CP was published in a clinical trial in 2011, and it has been known since 2015 that the analgesic effect of pregabalin on CP has a different mechanism of action than conventional analgesics. Currently, research is focused on combining pregabalin with antioxidants and on methods to predict the patient’s response to pregabalin administration. Based on current research, pregabalin appears to be a very useful agent for the pharmacologic treatment of pain in the setting of CP.
Citation
Gałązka J K, Skrzydło-Radomańska B, Kasztelan-Szczerbińska B, Cichoż-Lach H. Usage of pregabalin in the treatment of pain associated with chronic pancreatitis – a clinically oriented narrative review. Eur J Transl Clin Med. 2023;6(2):91-94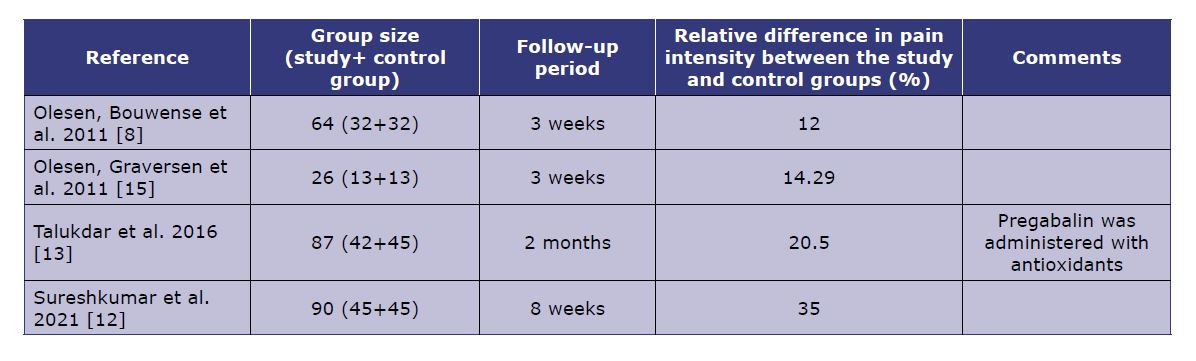

Introduction
Chronic pancreatitis (CP) is one of the most common gastroenterological diseases. In 2017, more than 1.5 million patients were diagnosed with de novo CP, compared to 1 million in 1990. In addition, Poland, along with Belgium and Slovakia, is one of the countries with the highest incidence of CP in the world [1]. According to the most recent definition, chronic pancreatitis is defined as a fibro-inflammatory syndrome of the pancreas, in which there is a persistent immune response associated with a damaging or stress factor, which manifests itself in individuals with a pre-existing genetic or environmental risk [2].
Abdominal pain (less often back pain) is one of the key symptoms of pancreatic diseases, including CP, the presence of which may precede both the loss of exocrine and endocrine function of this organ. Once disease remission is achieved and maintained, analgesia is a key element of patient management. The best-known algorithm is the so-called analgesic ladder, recommending starting with non-steroidal anti-inflammatory drugs (NSAIDs) and if not ineffective, escalate to weak and strong opioids [2].Currently, the use of surgical methods to reduce pain in patients with CP is being considered [3]. In some patients, the pain can be so severe that it leads to sleep disorders, depression and other mental disorders [4-6].
Co-analgesics may be added at any stage of analgesia. Anti-epileptic drugs have been used as co-analgesics for some time, among them pregabalin. According to the Summary of Product Characteristics (SmPC), treatment of pain with pregabalin can be initiated with a dose of 150 mg daily, administered in two or three divided doses, and then (according to the effects and tolerability of the drug, particularly renal function) the dose can be gradually increased up to up to 600 mg daily [7].
The aim of the article is to summarize the studies conducted so far on the use of pregabalin in patients suffering from pain in the course of chronic pancreatitis.
Material and methods
In order to collect articles on the topic, PubMed and Google Scholar databases were searched using the keywords “pregabalin,” “chronic pancreatitis” and their synonyms.
Results and discussion
The first data on the beneficial effect of pregabalin on pain in the course of CP was published in a 2011 clinical trial in which pregabalin was co-administrated with other analgesics, 36% of patients experienced relief compared to 24% in the placebo group [8]. Since then, more of similar clinical trials have been conducted, the results of which are summarized in Table 1.
In 2015, the results of a study were published showing that the mechanism of analgesic action of pregabalin in patients with CP differs from other agents used in pain management [9]. This implies that pregabalin may be particularly useful in treating patients who do not respond satisfactorily to conventional ladder-based treatment.
Observational studies have shown that one of the mechanisms of neuropathic pain in the course of CP is the adaptation of the structures of the central nervous system (CNS) caused by inflammation [10-11]. This led researchers to try to administer pregabalin together with antioxidant substances (e.g. methionine, selenium, β-carotene, ascorbic acid and α-tocopherol). Clinical trials on the simultaneous administration of pregabalin and antioxidants in patients with pain in the course of CP resulted in greater degree of pain reduction compared to those on pregabalin alone (Table 1) [12-13]. In another clinical trial, conducted on pediatric patients (average age 13 years), it was suggested that the administration of antioxidants (vitamin C, selenium) by itself reduces pain in 68% of patients [14].
Table 1. Summary of the results of clinical trials on the use of pregabalin in the treatment of pain in the course of CP; the VAS scale was used to assess pain in all of the above trials.
On the other hand, there are claims about the insufficient level of testing of pregabalin in the treatment of pain in the course of CP. The authors of a review from 2016 suggested that in previous studies, insufficient attention was paid to the long-term effects of pregabalin use in patients with CP and its overall impact of such therapy on their quality of life [16].
For some time, it was suspected that frequent diarrhea and changes in the intestinal mucosa typical of CP adversely affected the pharmacokinetics of pregabalin administered orally. These concerns were dispelled in an observational study from 2012, which reported that the pharmacokinetic profile of pregabalin in patients with CP was preserved and dose modification in such patients should be considered only in the case of renal failure [17]. However, it should be noted that according to pregabalin’s SmPC, its use in diabetes (a frequent secondary complication of pancreatic diseases) may disturb the bicarbonate balance and require an increase in the dose of hypoglycemic drugs in the patient, including insulin [7].
Due to the proven role of neuroplasticity in the development of pain in some patients with CP, and the frequent digestive system-related adverse effects of pregabalin, attempts have been made to construct methods predicting the response of patients to its use in pain management. In addition to EEG monitoring of analgesia (see below), Quantitative Sensory Testing (QST) may be used. The response was observed only after electrical stimulation of the Th10 dermatome (corresponding with the pancreas) and the effectiveness of such prediction was estimated at 83.9% [18-19].
When treating pain therapy in patients with impaired verbal contact (or unconscious), the level of analgesia can be tested using electroencephalography (EEG). After administration of pregabalin, the normalization of the (previously increased) amplitude of theta waves over the parietal lobes may be an indicator interpretable as analgesia [20].
Conclusion
According to the latest studies, including randomized clinical trials, pregabalin seems to be an effective analgesic in patients with CP. Its use should be considered primarily in patients in whom conventional measures of the analgesic ladder proved unsatisfactory. Pregabalin seems to have a synergistic effect with antioxidants and the degree of its absorption is not significantly affected by the course of CP itself. The patient’s response to pregabalin therapy can be predicted using QST, whereas in patients with impaired verbal contact it can be monitored using EEG.
Conflicts of interest
None
Sources of funding
None
----------------------
(Image source: www.istockphoto.com)
References
| 1. |
Ouyang G, Pan G, Liu Q, Wu Y, Liu Z, Lu W, et al. The global, regional, and national burden of pancreatitis in 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. BMC Med [Internet]. 2020;18:388. Available from: https://bmcmedicine.biomedcentral.com/articles/10.1186/s12916-020-01859-5.
|
| 2. |
Shimizu K, Ito T, Irisawa A, Ohtsuka T, Ohara H, Kanno A, et al. Evidence-based clinical practice guidelines for chronic pancreatitis 2021. J Gastroenterol [Internet]. 2022;57:709–24. Available from: https://doi.org/10.1007/s00535-022-01911-6.
|
| 3. |
Goulden MR. The pain of chronic pancreatitis: a persistent clinical challenge. Br J Pain [Internet]. 2013;7:8–22. Available from: http://journals.sagepub.com/doi/10.1177/2049463713479230.
|
| 4. |
Sarkar S, Sarkar P, M R, Hazarika D, Prasanna A, Pandol SJ, et al. Pain, depression, and poor quality of life in chronic pancreatitis: Relationship with altered brain metabolites. Pancreatology [Internet]. 2022;22:688–97. Available from: https://linkinghub.elsevier.com/retrieve/pii/S1424390322002022.
|
| 5. |
Tuck NL, Teo K, Kuhlmann L, Olesen SS, Johnson M, Bean DJ, et al. Pain patterns in chronic pancreatitis and chronic primary pain. Pancreatology [Internet]. 2022;22:572–82. Available from: https://linkinghub.elsevier.com/retrieve/pii/S1424390322001673.
|
| 6. |
Yadav D, Askew RL, Palermo T, Li L, Andersen DK, Chen M, et al. Association of chronic pancreatitis pain features with physical, mental, and social health. Clin Gastroenterol Hepatol [Internet]. 2022; Available from: https://linkinghub.elsevier.com/retrieve/pii/S1542356522009247.
|
| 7. |
Pregabalin Pfizer. Annex I. Summary of product characteristisc [Internet]. Eur. Med. Agency. 2019 [cited 2022 Jun 10]. Available from: https://www.ema.europa.eu/en/documents/product-information/pregabalin-pfizer-epar-product-information_en.pdf.
|
| 8. |
Olesen SS, Bouwense SAW, Wilder-Smith OHG, van Goor H, Drewes AM. Pregabalin reduces pain in patients with chronic pancreatitis in a randomized, controlled trial. Gastroenterology [Internet]. 2011;141:536–43. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0016508511004744.
|
| 9. |
Bouwense S, Olesen S, Drewes A, van Goor H, Wilder-Smith O. Pregabalin and placebo responders show different effects on central pain processing in chronic pancreatitis patients. J Pain Res [Internet]. 2015;375. Available from: http://www.dovepress.com/pregabalin-and-placebo-responders-show-different-effects-on-central-pa-peer-reviewed-article-JPR.
|
| 10. |
Ceyhan GO, Demir IE, Rauch U, Bergmann F, Müller MW, Büchler MW, et al. Pancreatic neuropathy results in “Neural Remodeling” and altered pancreatic innervation in chronic pancreatitis and pancreatic cancer. Am J Gastroenterol [Internet]. 2009;104:2555–65. Available from: https://journals.lww.com/00000434-200910000-00024.
|
| 11. |
Dimcevski G, Sami SAK, Funch-Jensen P, Le Pera D, Valeriani M, Arendt-Nielsen L, et al. Pain in Chronic Pancreatitis: The Role of reorganization in the central nervous system. Gastroenterology [Internet]. 2007;132:1546–56. Available from: https://linkinghub.elsevier.com/retrieve/pii/S001650850700176X.
|
| 12. |
Sureshkumar S, Omang A, Anandhi A, Rajesh BS, Abdulbasith KM, Vijayakumar C, et al. Efficacy of pregabalin and antioxidants combination in reducing pain in chronic pancreatitis: a double blind randomized trial. Dig Dis Sci [Internet]. 2021;66:4017–25. Available from: https://link.springer.com/10.1007/s10620-020-06711-7.
|
| 13. |
Talukdar R, Lakhtakia S, Reddy DN, Rao GV, Pradeep R, Banerjee R, et al. Ameliorating effect of antioxidants and pregabalin combination in pain recurrence after ductal clearance in chronic pancreatitis: Results of a randomized, double blind, placebo controlled trial. J Gastroenterol Hepatol [Internet]. 2016;31:1654–62. Available from: https://onlinelibrary.wiley.com/doi/10.1111/jgh.13332.
|
| 14. |
Gopan A, Srivastava A, Mathias A, Yachha SK, Jain SK, Mishra P, et al. Efficacy and predictors of pain response to combined antioxidants in children with chronic pancreatitis. Dig Dis Sci [Internet]. 2023;68:1500–10. Available from: https://link.springer.com/10.1007/s10620-022-07676-5.
|
| 15. |
Olesen SS, Graversen C, Olesen AE, Frøkjaer JB, Wilder-Smith O, van Goor H, et al. Randomised clinical trial: pregabalin attenuates experimental visceral pain through sub-cortical mechanisms in patients with painful chronic pancreatitis. Aliment Pharmacol Ther [Internet]. 2011;34:878–87. Available from: https://onlinelibrary.wiley.com/doi/10.1111/j.1365-2036.2011.04802.x.
|
| 16. |
Gurusamy KS, Lusuku C, Davidson BR. Pregabalin for decreasing pancreatic pain in chronic pancreatitis. Cochrane Database Syst Rev [Internet]. 2016;2016. Available from: http://doi.wiley.com/10.1002/14651858.CD011522.pub2.
|
| 17. |
Olesen AE, Olofsen E, Olesen SS, Staahl C, Andresen T, Dahan A, et al. The Absorption profile of pregabalin in chronic pancreatitis. Basic Clin Pharmacol Toxicol [Internet]. 2012;111:385–90. Available from: https://onlinelibrary.wiley.com/doi/10.1111/j.1742-7843.2012.00914.x.
|
| 18. |
Bouwense SAW, Olesen SS, Drewes AM, Poley J-W, van Goor H, Wilder-Smith OHG. Effects of pregabalin on central sensitization in patients with chronic pancreatitis in a randomized, controlled trial. Eldabe S, editor. PLoS One [Internet]. 2012;7:e42096. Available from: https://dx.plos.org/10.1371/journal.pone.0042096.
|
| 19. |
Olesen SS, Graversen C, Bouwense SAW, van Goor H, Wilder-Smith OHG, Drewes AM. Quantitative sensory testing predicts pregabalin efficacy in painful chronic pancreatitis. Miaskowski C, editor. PLoS One [Internet]. 2013;8:e57963. Available from: https://dx.plos.org/10.1371/journal.pone.0057963.
|
| 20. |
Graversen C, Olesen SS, Olesen AE, Steimle K, Farina D, Wilder-Smith OHG, et al. The analgesic effect of pregabalin in patients with chronic pain is reflected by changes in pharmaco-EEG spectral indices. Br J Clin Pharmacol [Internet]. 2012;73:363–72. Available from: https://onlinelibrary.wiley.com/doi/10.1111/j.1365-2125.2011.04104.x.
|
