

Del Nido cardioplegia versus other contemporary solutions for myocardial protection – a literature review


Abstract
Myocardial protection is one of the most important factors ensuring patient safety during cardiac surgery with the application of cardiopulmonary bypass. Infusion of cardioplegic solution into the coronary circulation protects the heart and provides a standstill operating field for the surgeon. Cold blood cardioplegia and crystalloid cardioplegia are the two main types of solutions with a long history of use and a large amount of research proving their efficacy and safety. Relatively new del Nido cardioplegia seems to be an interesting alternative. We reviewed the literature comparing del Nido cardioplegia with two other types of cardioplegic solutions. We took into consideration many different clinical and biochemical aspects may indicate the quality of cardioprotection.
Citation
Brzeska B, Karolak W, Żelechowski P, Łoś A, Ulatowski N, Pawlaczyk R. Del Nido cardioplegia versus other contemporary solutions for myocardial protection – a literature review. Eur J Transl Clin Med. 2023;6(1):41-57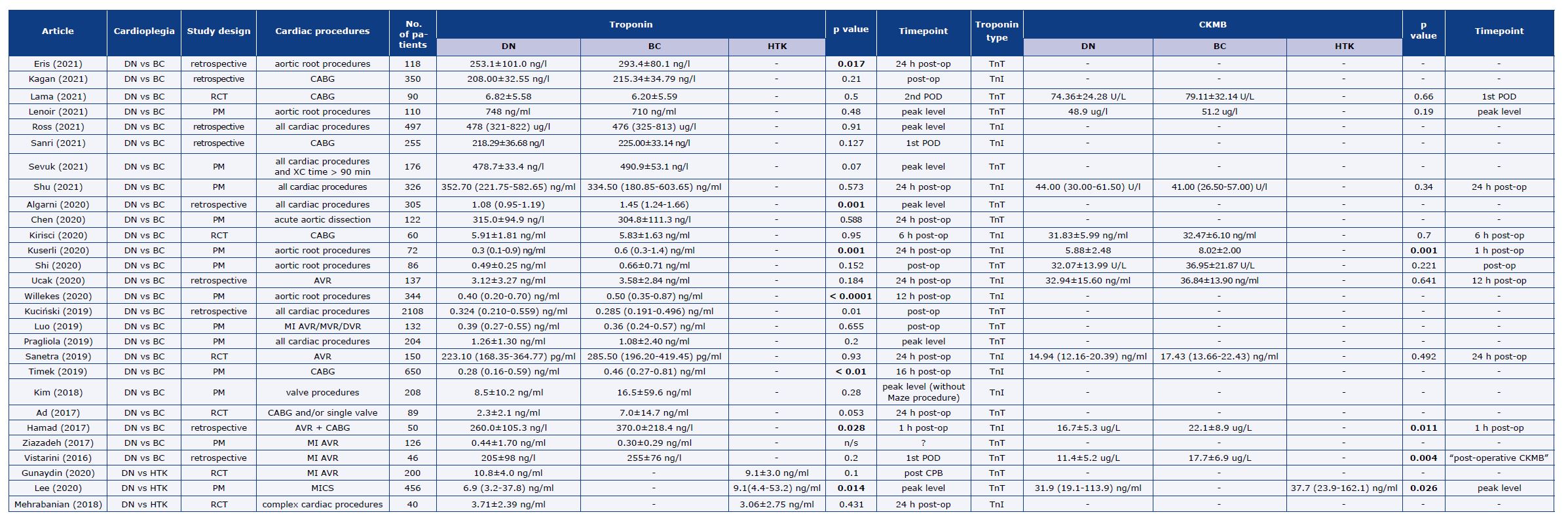




















Introduction
Effective myocardial protection is crucial for a successful outcome of cardiac surgery with the application of cardiopulmonary bypass (CPB). For nearly 50 years the most common method of cardioprotection has been the infusion of cardioplegic solution into the coronary vessels. This provides a bloodless and motionless operating field which is perfect for precise surgery, however with a time limit resulting from the principles of physiology and biochemistry. The safe ischemic time varies depending on the composition and temperature of the cardioplegic solution. Some of the warm blood infusions must be delivered continuously, whereas a single infusion of some cold crystalloid solutions provide over two hours of secure myocardial protection during cross-clamping (XC) of the aorta. Thanks to research we have a much better understanding of the mechanism of ischemia-reperfusion injury (IRI) and better ways to prevent it.
Cardioplegia is a name given to a group of solutions using different mechanisms to arrest the heart in diastole with additives for cell membrane stabilization or oedema prevention. The mechanism of each is the result of a characteristic composition (Table 1). The development of high-potassium blood cardioplegia was a milestone in cardiac surgery. However, short intervals between doses are its weak point, particularly in the current era of minimally invasive cardiac procedures. Whereas the low-sodium crystalloid solution provides a very long working interval and rarely has to be re-dosed, however the long reperfusion time is a disadvantage. Del Nido cardioplegia (DNC) solution derived from pediatric cardiac surgery combines the most important aspects of the high-potassium and low-sodium cardioplegia solutions making it an interesting alternative for adult patients. Despite the growing number of studies and meta-analysis, there are no guidelines or consensus regarding which cardioplegic solution is the most beneficial.
Table 1. Cardioplegia solutions composition
CBC – cold blood cardioplegia, DNC – Del Nido cardioplegia, HTK – Bretschneider histidine-tryptophan-ketoglutarate solution
Material and methods
For this review, we included retrospective and prospective studies comparing DNC with cold blood cardioplegia (CBC) of any kind or crystalloid cardioplegia (Bretschneider histidine-tryptophan-ketoglutarate solution (HTK)). We searched the MEDLINE database for English-language articles using the following keywords: “del Nido cardioplegia,” “del Nido vs cardioplegia” and “cardioplegia AND del Nido”. We looked for articles on standard adult cardiac procedures (single valve or coronary artery bypass grafting (CABG)) and combined procedures (multivalve, reoperations, aortic root). After evaluation of the substantive value of abstracts, full-text articles were analyzed. The analyzed studies concerned a total of 9839 cases, including 5073 with del Nido cardioplegia. Experimental, animal-model, pediatric and modified del Nido studies were excluded (Figure 1). Results from selected studies are collected and presented in the form of tables with an indication of the number of included patients, the type of surgery and study design (prospective, retrospective and retrospective with propensity-score matching (PSM)).
Figure 1. Literature search flow chart
Results
Cardiopulmonary bypass and cross-clamp times
Significant shortening of the CPB and XC times in the DNC groups compared with CBC was described in most of the analyzed studies [1-17] (Table 2). Four studies [18-21] reported shorter XC times without a change in the CPB time. This may confirm that surgery is performed smoothly when DNC is used but may suggest the necessity of a longer reperfusion or lidocaine residual effect with delayed activation of the conductive system. Compared with HTK, there were no reported differences in CPB or XC times. This might be due to the fact that only one dose of cardioplegia was usually needed in both groups.
Table 2. CPB and XC times
* Not significant due to alpha < 0.001
Cardiac enzymes
In the majority of analyzed articles, the postoperative levels of cardiac enzymes (creatine phosphokinase myocardial band (CK-MB), troponin T or I (TnT and TnI), depending on study protocol) were similar or lower when DNC was compared with CBC cases (Table 3; download here). Different results were shown in the subgroup analysis of aortic root cases [2] with XC time > 180 min where CK-MB levels were significantly higher in the DNC group. Significantly higher postoperative TnT levels in the DNC group were reported also in a retrospective study of 2108 cardiac cases of all types [10]. However, a more thorough analysis revealed that uneven distribution of surgery types (resulting in longer CPB and XC times in DNC) and preoperative TnT level was responsible for that result. In two studies comparing DNC with HTK cardiac enzymes were comparable [22-23] between the groups.
Table 3. Postoperative Tn and CK-MB levels
Two other studies on DNC vs. HTK suggested a higher level of cardiac enzymes in cases when DNC was used with longer XC. Lee et al. [24] showed lower peak TnI and CK-MB in DNC. A peak level of cardiac enzymes according to the XC time was also lower in DNC, but the differences between groups tended to decrease with a crossover point of 100 minutes of XC. In a sub-analysis of cases with a second cardioplegia dose, Gunaydin et al. showed significant differences in TnT levels measured during weaning from CPB to the disadvantage of DNC [25].
Cardiac activity and return to sinus rhythm
The quality of myocardial protection may be also estimated by observing the electrical and mechanical activity of the arrested heart: satisfactory protection is shown by no such activity before the clamp removal and reperfusion. Ucak et al. [8] reported ventricular fibrillation (VF) during XC in 5.7% of cases in DNC and 9.4% in the CBC group (p = 0.016). In the RCT by Sanetra et al. [26] no differences between groups in terms of electrical activity during XC were observed. In majority of the studies, patients with DNC more often had a spontaneous return of sinus rhythm (SR) return and less often needed electric defibrillation, compared to those with CBC (Table 4). When compared with HTK, only one study [23] reported a rate of spontaneous SR return. It was significantly higher in the DNC group and even more pronounced in a subgroup of cases with XC > 120 min (93.1% vs 42.3%). A very high number of VF in the HTK groups raises some questions.
Table 4. Rate of electric defibrillation
Cardioplegia volume and blood product transfusion rates
In the majority of reviewed studies, total cardioplegia volume was significantly higher in the CBC than in the DNC cases [1, 4-6, 8-9, 11, 15, 17-18, 20, 26-33]. In only one study this volume was lower in CBC patients [21]. When only crystalloid volume is taken into consideration, higher volume was administered to patients who received DNC [1, 14, 31, 34-35]. The differences in administered volume did not seem to affect the postoperative hematocrit (HCT) levels. This parameter was analyzed in 10 articles and 6 of them reported comparable HCT levels between DNC and CBC [9, 11, 27-28, 31, 34]. In the other four studies, HCT was higher in the DNC group [6, 14, 18, 36].
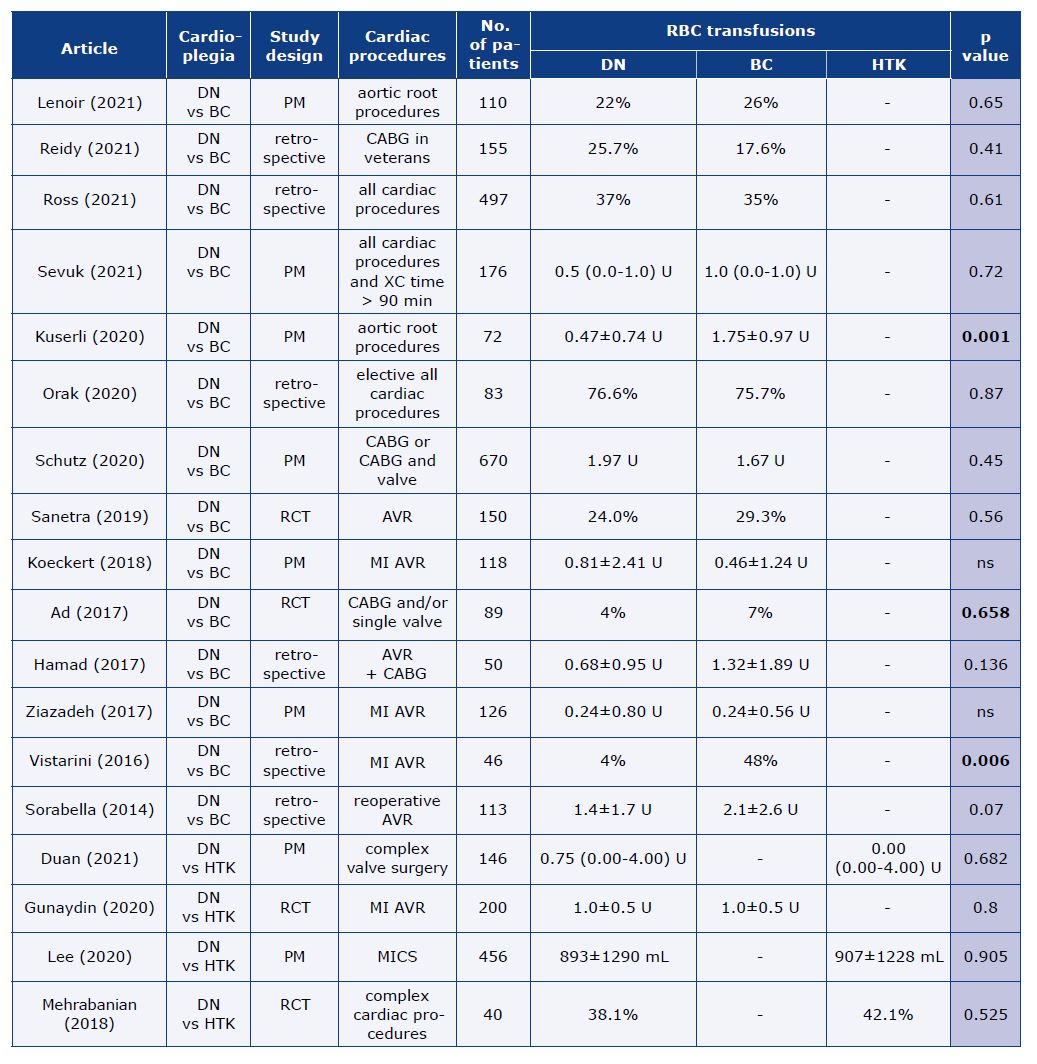
The amount of transfused blood and blood products was similar in the majority of studies comparing DNC and CBC. Due to the lack of homogeneity in reporting between articles in Table 5, we present only data about red blood cell (RBC) transfusions. Three studies [6, 18, 34] showed a higher need for different kinds of blood products in the CBC group. When DNC was compared with HTK, haemoglobin levels as well as the rate of transfusions during CPB and in the postoperative period were comparable between the groups [22, 24-25]. Only Duan et al. [23] reported a higher need for platelet concentrates (PC), fresh frozen plasma and cryoprecipitate in the HTK group. In the subgroup analysis of cases with XC > 120 minutes, only differences in PC remain significant.
Table 5. RBC transfusions
Heart rhythm disturbances in the postoperative period
The majority of reviewed articles showed comparable results between DNC and CBC in terms of postoperative atrial fibrillation (AF) occurrence (Table 6). Only Timek et al. [11] reported a higher rate of AF after isolated CABG with DNC. Opposite results with a higher rate of AF in CBC cases were shown in the two studies. The first of which [20] showed a correlation between the occurrence of AF and cardioplegia volume in patients who underwent isolated CABG. In the second study, [37] patients who underwent CABG with or without valve intervention had a higher rate of AF, atrial flutter and VT in cases with CBC in all analyses excluding subgroups with left ventricular ejection fraction (LVEF) < 35%.
Table 6. Postoperative AF occurrence
Shu et al demonstrated a comparable rate of AF but higher risk of ventricular rhythm disturbances was shown in PSM analysis as well as in sub-analysis of cases with XC > 69 minutes [38]. In log regression analysis DNC had a significant effect on reduction in the rate of ventricular arrhythmias.
The need for a temporary pacemaker was equal [39] or higher in DNC groups [40] when compared with CBC.
Two studies comparing DNC with HTK presented results on postoperative arrhythmia. Gunaydin et al. [25] reported a higher rate of AF and atrioventricular (AV) block in the general cohort and subgroup with a second cardioplegia dose when DNC was used. When only one dose was administered, the results were comparable. Different results were reported by Duan et al. [23]. 3rd degree AV block, VF and sudden cardiac arrest were more frequent in the HTK group. However, in the logistic regression model, the type of cardioplegia did not have a statistically significant influence on the occurrence of severe post-operative arrhythmia. No differences were found in a sub-analysis of cases with XC > 120 minutes.
Inotropic/vasoactive support and low cardiac output syndrome
Due to heterogeneity in reporting it is difficult to show and analyze differences in the need for inotropic/vasopressor support. Only Orak et al. [27] report lower noradrenaline (NA) requirements during surgery when CBC was used. Seven of reviewed articles showed a lower need for inotropic/ vasopressor support in the DNC group [2, 4, 7-8, 11, 15, 18]. In Ad et al. [31] the need for inotropic support was also lower in the DNC group, but significance was not reached due to an alpha level of p < 0.001. A total of 19 other articles reported no differences in terms of the need for inotropic/ vasoactive and rate of low cardiac output syndrome (LCOS) between DNC and CBC. Three [22, 24-25] of a total of four studies comparing DNC and HTK showed no differences in the need for inotropic support. Only in one sub-analysis of cases with XC < 120 minutes from the study by Duan et al. [23] the doses of NA were lower in the DNC group.
Non-cardiac or systemic complications
Ross et al. [30] showed no differences in the rate of acute kidney injury (AKI), stroke or composite death. However, the risk of reoperation caused by bleeding was higher in the DNC group. In the sub-analysis of CABG cases the post-operative levels of creatinine were significantly lower in the DNC group but so were the pre-operative levels. A RCT by Santera et al. [26] reported that the rate of significant creatinine increase (> 25% or > 0.5mg/dL) or AKI was greater in the CBC group. The retrospective study by Eris et al. [18] also showed that AKI was more frequent in the CBC group. Further analysis revealed it only applies to the AKI Stage 1. There were no differences in the rate of other complications (cerebrovascular incident, infection, AF, bleeding, respiratory failure) or mortality. Stage 1 AKI (or any AKI) in CBC was also more frequent in a retrospective study by Kagan et al. [21] In logistic regression analysis AKI was correlated, among others, with increased cardioplegia volume.
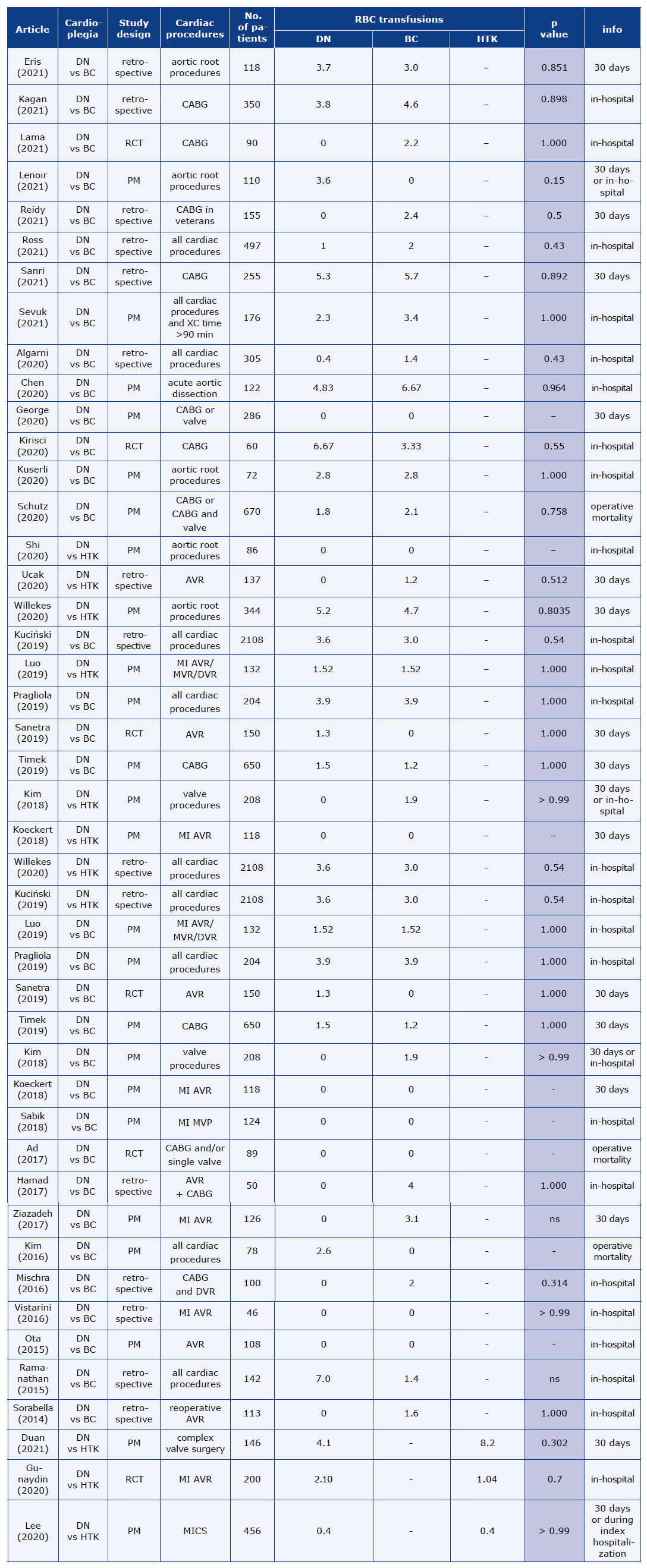
Luo et al. [33] showed significantly lower levels of blood urea nitrogen (BUN) in the DNC group, without differences in the post-operative levels of creatinine, eGFR or pre-operative BUN. However, the DNC group had a significantly lower Euro SCORE II. Schutz et al. [37] reported a significantly higher rate of neurological complications in the postoperative period in DNC for the overall cohort (CABG + valve procedure), as well as for the subgroup with LVEF < 35%. The rate of stroke was also significantly higher in this subgroup when DNC was used. The frequency of total infections and total sternal infections was greater in the CBC group for the overall cohort. Overall, most studies did not reveal differences in the rate of postoperative complications between groups. It is noteworthy that almost all of the reviewed articles analyzed different kinds of complications with different definitions. Early mortality was the complication that was most often studied (in 37 studies, see Table 7) [1-6, 8-21, 23-26, 28-35, 37, 39-42].
Table 7. Early mortality
Echocardiographic findings
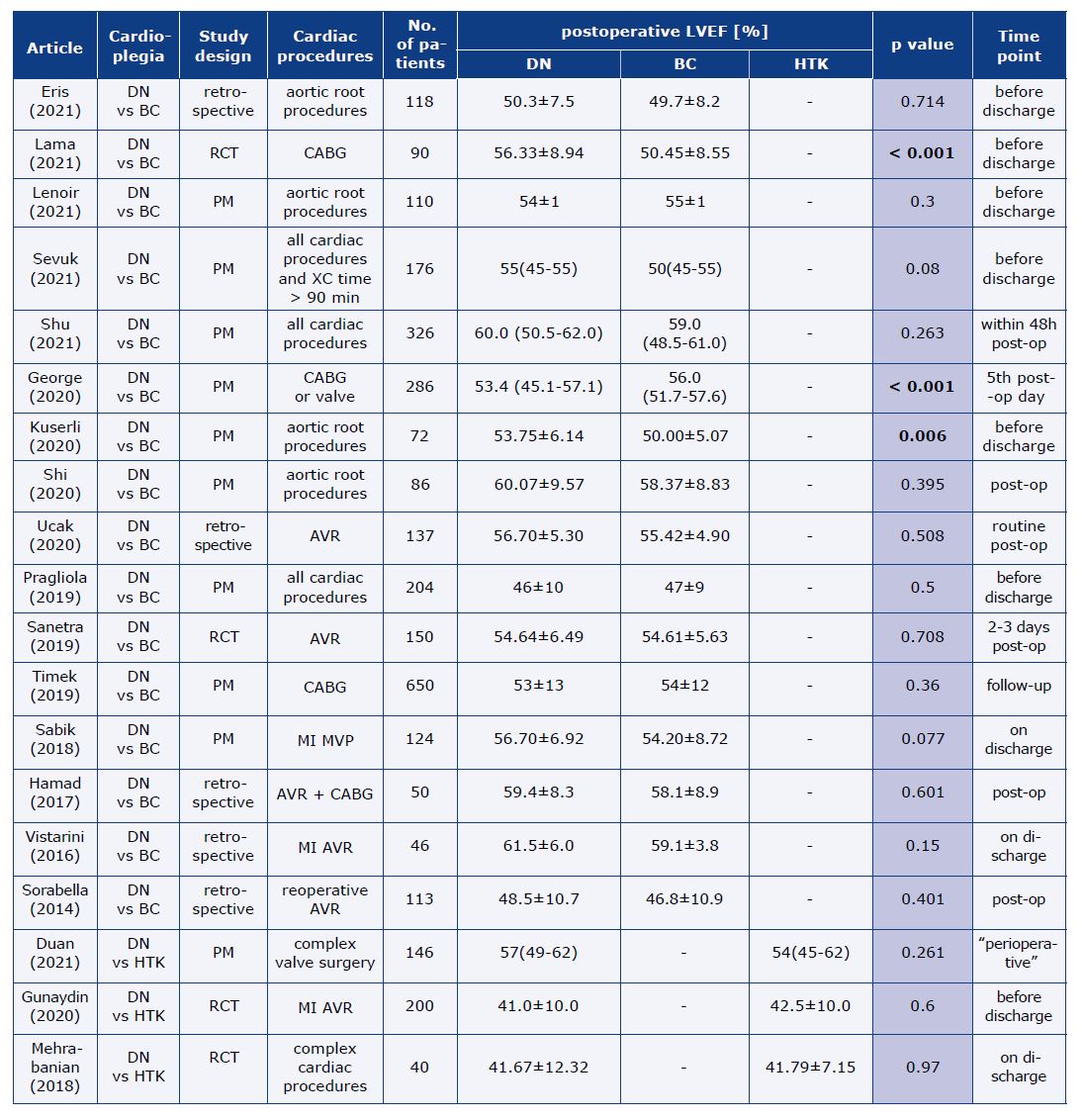
Only George et al. [39] reported significantly lower LVEF measured on the 5th post-operative day (POD) in the DNC group, although the median values in both groups were in the normal range.
Four [1, 6, 16, 36] studies (including one RCT), all describing different types of cardiac surgeries, showed better echocardiographic parameters in the DNC group measured at different time points during hospitalization. No differences were shown in other studies comparing DNC and CBC (Table 8).
Table 8. LVEF
Two RCTs on DNC versus HTK [22, 25] reported no differences in the LVEF measured before discharge. In the study by Mehrebenian et al. [22], LVEF measured in the OR after weaning from CPB was also comparable. In Duan et al. [23] LVEF measured in the postoperative period was also similar between groups, however systolic volume and cardiac output (as echocardiographic parameters) were significantly lower in HTK, both in the general cohort and subgroup of XC ≥ 120 minutes. Whereas the sub-analysis of cases with XC < 120 minutes showed no differences. [23].
Length of ICU and hospital stay, mechanical ventilation time
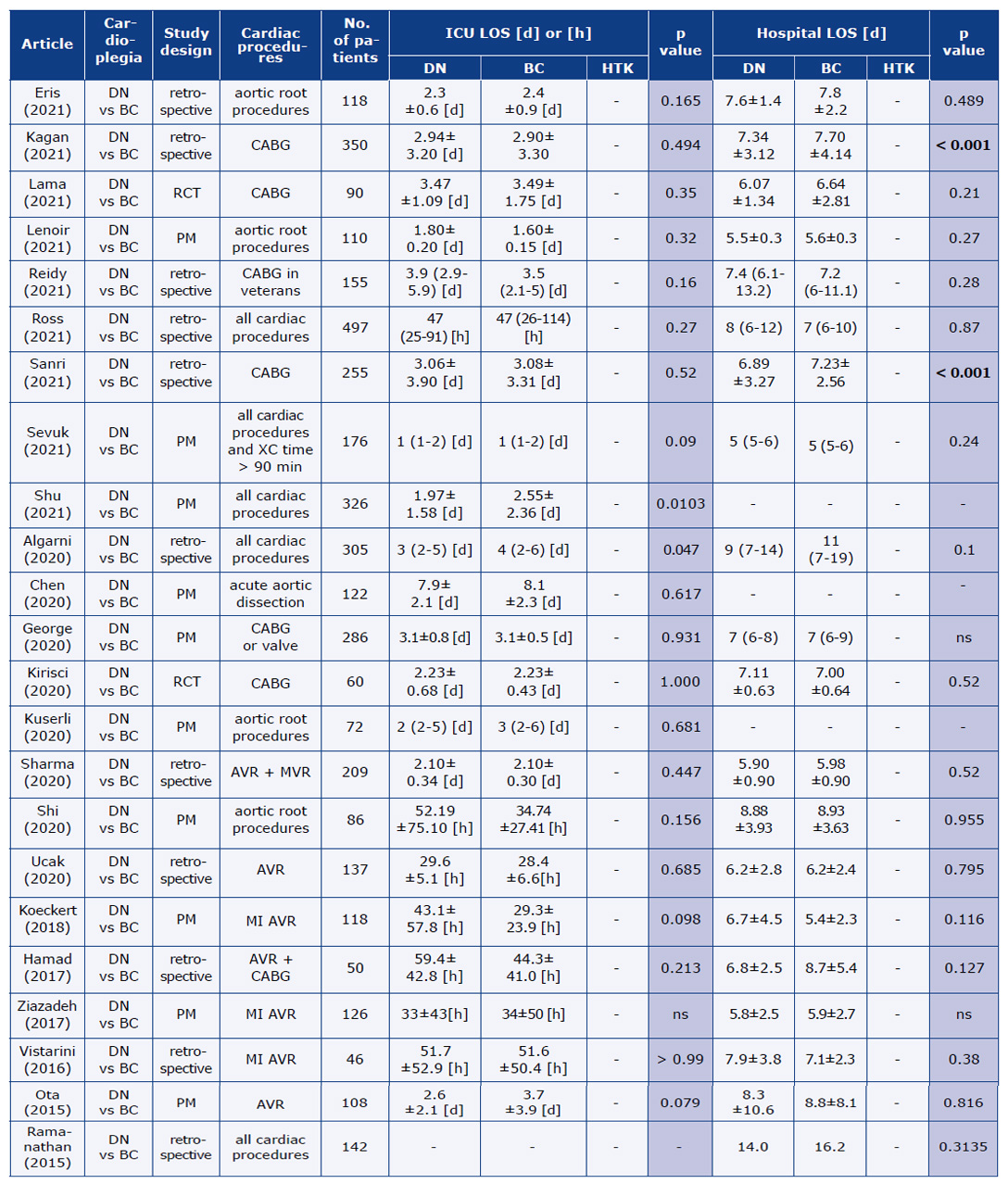
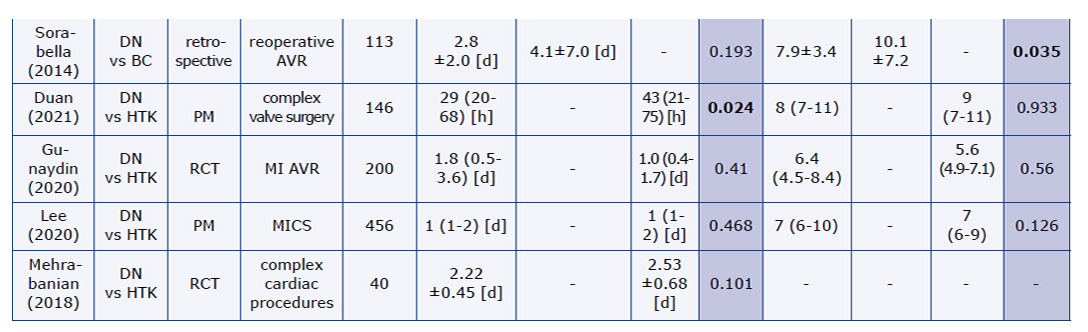
The majority of articles presented comparable hospital and intensive care unit (ICU) length of stay (LOS) (Table 9) and time of mechanical ventilation between the DNC and CBC cases. A shorter ICU stay for the DNC group was reported in 2 studies [4, 38], with patients undergoing all types of cardiac procedures. In their study concerning AVR reoperations, Sorabella et al. [29] reported no differences in the ICU LOS and mechanical ventilation time, although hospital LOS was significantly shorter when DNC was used. Similar results can be found in two retrospective studies on isolated CABG [20-21]. Significantly shorter mechanical ventilation time in the CBC group was reported by Vistarini et al. [34]. In a sub-analysis of cases with longer XC time requiring a second DNC or HTK dose, Gunaydin et al. [25] reported significantly longer ICU LOS and hospital LOS in the DNC group. No differences were shown when only one dose of either DNC or HTK was used. Mechanical ventilation time was comparable in all analyses. Duan et al. [23] observed that the ICU LOS was significantly shorter in the DNC group, both in the general cohort after PSM and in the sub-analysis of cases with XC < 120 minutes. In XC ≥ 120 minutes cases ICU LOS was comparable between groups. None of the sub-analyses in that study revealed differences in the hospital LOS.
Table 9. Hospital and ICU LOS
Discussion
All of the currently used cardioplegic solutions are safe and well-designed. The oldest of them, high-potassium CBC, is also the most widely used in the world [43]. CBC has great buffering properties and ensures cardiac arrest in a highly oxygenated environment. Its oncotic properties prevent cell oedema and its twenty minutes re-dosing period provides re-oxygenation and washout of waste products, which improves the preservation of ATP [39]. DNC developed by the team from Boston Children’s Hospital [44] is also a high-potassium solution. The main purpose of its chemical composition was to ensure the lowest possible intracellular accumulation of calcium, which is particularly elevated in depolarizing cardiac arrest. Depolarization creates higher sodium and calcium gradient, which leads to cell calcium overload – the main factor of IRI. Calcium influx is one of the mechanisms leading to mitochondrial dysfunction and reperfusion fibrillation [23].
High potassium levels may also lead to vasoconstriction and disrupt the endothelium function in coronary and peripheral vessels aggravating the damage during reperfusion [45]. DNC contains lidocaine (a Na+ -K+ pump blocker) which counteracts the unfavourable effects of depolarization by stabilizing the cell membrane, lowering excitability and elongating the refraction period [46]. All these actions reduce the probability of hypercontraction due to high Ca2+ concentration. What is more DNC itself contains a small amount of Ca2+. Additionally, lidocaine has a protective effect on the endothelium.
In some cardioplegia strategies, lidocaine can be administered into the peripheral circulation [31], however, it is more effective when injected directly into the coronary circulation. Unlike CBC, DNC has low nutritional value due to the small amount of blood and glucose. On the other hand, a small amount of blood leads to lower hematocrit (ca. 6-7%), which compared to CBC (ca. 26-32%) may provide better distribution in the coronary microcirculation. Such lower hematocrit could be beneficial, particularly in low temperatures when blood viscosity increases.
Better distribution means better cardioprotection and lower postoperative cardiac enzymes. HTK acts differently from the two above-mentioned solutions. A low-sodium solution causes membrane hyperpolarization, which leads to a reversible diastolic arrest. Better cell membrane stabilisation provides lower permeability for ions such as Ca2+. An additive of Mg2+ in HTK also stabilizes cardiomyocyte cell membranes, yet lidocaine seems to be superior and more effective.
Quality of cardioprotection: cardiac enzymes
Cardiac enzymes are one of the most reliable markers of cardioprotection during the cardiac surgery procedure. Elevated postoperative Tn or CK-MB level correlates with early outcomes and mortality of cardiac surgery patients. The majority of analyzed studies showed equally good or better cardioprotection in DNC cases when correlated with cardiac enzyme levels. The weak point is again the heterogeneity of reporting. Study protocols differ in terms of the time point of collecting blood samples, the measurement՚s accuracy over time [47], application and degree of hypothermia, cardioplegia administration and redosing protocols.
Quality of cardioprotection: post cross-clamp ventricular fibrillation
An indirect sign of cardioprotection is the heart՚s electrical activity during the procedure. In two studies analyzing this parameter, DNC was more effective in lowering the electrical activity of the heart.
Spontaneous return of SR after cross-clamp removal also gives information about cardioprotection. Longer ischemia and lower quality of cardioprotection increase the probability of VF and the need for defibrillation. Once again, the reported values are not homogeneous but are enough to make some conclusions. What draws attention is a significantly higher percentage of spontaneous SR return in DNC groups in the vast majority of the analysed studies. This illustrates good cardioprotection and control of Ca2+ accumulation mechanisms in cardiomyocytes, which is a main factor of VF after XC [42].
Hypothermia prolongs repolarization and is a known pro-arrhythmic factor. Constant cooling of the myocardium during many CBC repetitions may trigger VF. Slow rewarming of the heart after only one dose of DNC could be a protective factor [26]. However, this effect is not visible in HTK (also a single-dose cardioplegia solution) and probably plays an additional role in cardioplegia composition.
Less VF after XC removal means less direct current shocks and less myocardial damage, which may lower the concentrations of post-operative cardiac enzymes. Discrepancies in the VF:SR ratio noted in the studies may be due to the differences in the cardioplegia administration protocols or the patient population.
Quality of cardioprotection: echocardiographic parameters
Decreased contractility in the post-operative period may be the result of poor cardioprotection. All but one study [39] showed similar or better cardiac function in echocardiographic examination in the DNC groups when compared with CBC or HTK. It is noteworthy that not all of the articles analyzed changes between pre- and post-operative examinations. Duan et al. [23] comparing DNC and HTK reported better post-operative systolic volume and cardiac output measured by echocardiography in the former. However, this ratio does not necessarily indicate better heart function, only an increase in extracellular fluid. There is no evidence that LV mass influences cardioprotection [12]. However, LV hypertrophy and the presence of coronary disease in adults may have a negative effect the quality of cardioprotection in comparison with the pediatric population. Hypertrophied myocardium has a metabolism similar to that of fetal myocardium (increased glycolysis, reduced oxidation of fatty acids), which leads to reduced ischemia tolerance. This may suggest a better effect of DNC developed for similar conditions.
Postoperative complications
There is no evidence that the use of DNC reduces the number of postoperative complications. A relatively small number of analyzed cases may cause problems with obtaining statistical significance of rare complications. Differences in reporting also make it difficult to draw clear conclusions, as in the case of vasoactive or inotropic agent administration. LCOS may be a consequence of inadequate cardioprotection requiring vasoactive/inotropic support or even mechanical circulatory support. Almost every study had a different method of reporting data, thus making it difficult to compare them. However, in general patients with DNC had a similar or even lower need for vasoactive and inotropic agents.
The possible indirect influence of DNC on renal function is noteworthy. In four studies the DNC patients had better renal parameters [26, 33] or less frequent occurrence of AKI [18, 21, 26]. In studies by Eris and Kagan, this only applied to stage 1 AKI [18, 21]. Sanetra et al. hypothesized that lidocaine as a vasodilator could improve renal flow which in addition to shorter CPB and better cardiac function in the postoperative period may have a positive effect on kidney function [26]. A trend towards better renal function is also seen in metanalysis by Misra et al. [48].
Questions and limitations of the review
Two main DNC dosing protocols can be found in the literature. The first method is a constant volume (usually 1000 or 1500 ml) delivered regardless of the patient՚s body weight. The second approach is dosing based on the patient’s body weight (typically 20 mL/kg), with or without an indication of the maximum dose.
However, the method of administering the additional DNC doses remains unclear due to the lack of a standard dosing schedule. The most common rule is re-dosing ½ of the initial DNC dose after 60 minutes of XC if the expected total XC time is > 90 minutes. Many modifications to the re-dosing period or the volume and composition of the second DNC dose can be found in the literature [49-52]. The authors of the analyzed studies did not always include the protocols for administration and re-dosing of DNC. Those potential differences in dosing may be responsible for inconsistent results, particularly because the vast majority of the reviewed articles were retrospective.
Conclusions
The currently used cardioplegic solutions are safe and have proven properties to protect the heart against the effects of ischemia during open-heart surgery. The differences between DNC, CBC and HTK described in the analyzed studies do not disqualify any of the solutions but may suggest the need for further research, particularly in the context of longer XC times. More randomized trials are needed, possibly also examining cardiac function in a long-term follow-up.
Acknowledgements
None.
Funding
None.
Conflicts of interest
The authors do not have any conflict of interest in this project.
References
| 1. |
Moktan Lama PB, Khakural P, Sigdel S, Raj Bhatta M, Sah Teli R, Baral RK, et al. Del Nido Cardioplegia in Coronary Artery Bypass Grafting Surgery: A safe, efficacious and economic alternative to St. Thomas solution; an experience from a developing nation. Perfusion 2021;36(5):470-5. Available from: https://doi.org/10.1177/0267659121991033.
|
| 2. |
Lenoir M, Bouhout I, Jelassi A, Cartier R, Poirier N, El-Hamamsy I, et al. Del Nido cardioplegia versus blood cardioplegia in adult aortic root surgery. J Thorac Cardiovasc Surg. 2021;162(2):514-22.e2. Available from: https://doi.org/10.1016/J.JTCVS.2020.01.022.
|
| 3. |
Reidy MR, Jimenez E, Omer S, Cornwell LD, Runbeck SX, Preventza O, et al. Single-dose del Nido cardioplegia compared with standard cardioplegia during coronary artery bypass grafting at a Veterans Affairs Hospital. Tex Heart Inst J. 2021;48(1):e196981. Available from: https://doi.org/10.14503/THIJ-19-6981.
|
| 4. |
Algarni KD. Routine use of del Nido cardioplegia compared with blood cardioplegia in all types of adult cardiac surgery procedures. J Card Surg. 2020;35(12):3340-6. Available from: https://doi.org/10.1111/JOCS.15060.
|
| 5. |
Kirişci M, Koçarslan A, Altintaş Aykan D, Alkan Baylan F, Doğaner A, Orak Y. Evaluation of the cardioprotective effects of crystalloid del Nido cardioplegia solution via a rapid and accurate cardiac marker: heart-type fatty acid-binding protein. Turk J Med Sci. 2020;50(4):999-1006. Available from: https://doi.org/10.3906/SAG-2002-53.
|
| 6. |
Kuserli Y, Turkyilmaz S, Turkyilmaz G, Kavala AA. Comparison of del Nido cardioplegia and blood cardioplegia in aortic root surgery. Heart Surg Forum. 2020;23(3):E376-84. Available from: https://doi.org/10.1532/HSF.2861.
|
| 7. |
Sharma A, Dixit S, Mittal S, Sharma M, Sharma D, Mawar KK. Del Nido cardioplegia versus St Thomas cardioplegia solution in double valve replacement: a single centre experience. Perfusion 2021;36(5):476-81. Available from: https://doi.org/10.1177/0267659120961921.
|
| 8. |
Ucak HA, Ucak D. Single-Dose Del Nido cardioplegia vs. blood cardioplegia in aortic valve replacement surgery. Braz J Cardiovasc Surg. 2021;36(2):229-36. Available from: https://doi.org/10.21470/1678-9741-2020-0063.
|
| 9. |
Willekes H, Parker J, Fanning J, Leung S, Spurlock D, Murphy E, et al. Del Nido cardioplegia in ascending aortic surgery. Semin Thorac Cardiovasc Surg. 2021;35(1):33-41. Available from: https://doi.org/10.1053/J.SEMTCVS.2021.10.008.
|
| 10. |
Kuciński J, Górska A, Deja MA. Del Nido cardioplegia as a safe and effective method of myocardial protection in adult patients undergoing cardiac surgery: a single center experience. Kardiol Pol. 2019;77(11):1040-6. Available from: https://doi.org/10.33963/KP.14964.
|
| 11. |
Timek TA, Beute T, Robinson JA, Zalizadeh D, Mater R, Parker JL, et al. Del Nido cardioplegia in isolated adult coronary artery bypass surgery. J Thorac Cardiovasc Surg. 2020;160(6):1479-85.e5. Available from: https://doi.org/10.1016/j.jtcvs.2019.09.027.
|
| 12. |
Kim WK, Kim HR, Kim JB, Jung SH, Choo SJ, Chung CH, et al. del Nido cardioplegia in adult cardiac surgery: beyond single-valve surgery. Interact Cardiovasc Thorac Surg 2018;27(1):81-7. Available from: https://doi.org/10.1093/ICVTS/IVY028.
|
| 13. |
Sabik JF, Raza S, Chavin KD. Safety and benefits of new techniques and technologies in less invasive mitral valve repair. J Card Surg. 2018;33(10):609-19. Available from: https://doi.org/10.1111/JOCS.13801.
|
| 14. |
Hamad R, Nguyen A, Laliberté É, Bouchard D, Lamarche Y, El-Hamamsy I, et al. Comparison of del Nido Cardioplegia With Blood Cardioplegia in Adult Combined Surgery. Innovations (Phila) 2017;12(5):356-62. Available from: https://doi.org/10.1097/IMI.0000000000000403.
|
| 15. |
Ziazadeh D, Mater R, Himelhoch B, Borgman A, Parker JL, Willekes CL, et al. Single-dose del Nido cardioplegia in minimally invasive aortic valve surgery. Semin Thorac Cardiovasc Surg. 2017;29(4):471-6. Available from: https://doi.org/10.1053/J.SEMTCVS.2017.10.001.
|
| 16. |
Mishra P, Jadhav RB, Mohapatra CKR, Khandekar J, Raut C, Ammannaya GK, et al. Comparison of del Nido cardioplegia and St. Thomas Hospital solution – two types of cardioplegia in adult cardiac surgery. Kardiochir Torakochirurgia Pol. 2016;13(4):295-9. Available from: https://doi.org/10.5114/KITP.2016.64867.
|
| 17. |
Ota T, Yerebakan H, Neely RC, Mongero L, George I, Takayama H, et al. Short-term outcomes in adult cardiac surgery in the use of del Nido cardioplegia solution. Perfusion 2016;31(1):27-33. Available from: https://doi.org/10.1177/0267659115599453.
|
| 18. |
Eris C, Engin M, Erdolu B, Kagan As A. Comparison of del Nido Cardioplegia vs. blood cardioplegia in adult aortic surgery: Is the single-dose cardioplegia technique really advantageous? Asian J Surg. 2022;45(2):1122-7. Available from: https://doi.org/10.1016/J.ASJSUR.2021.09.032.
|
| 19. |
Sevuk U, Dursun S, Ar ES. Propensity-Matched Analysis of Del Nido Cardioplegia in Adults Undergoing Cardiac Surgery with Prolonged Cross-Clamping Time. Braz J Cardiovasc Surg 2021;37(5):702-9. Available from: https://doi.org/10.21470/1678-9741-2020-0309.
|
| 20. |
Sanri US, Özsin KK, Toktaş F, Yavuz Ş. Comparison of Del Nido cardioplegia and blood cardioplegia in terms of development of postoperative atrial fibrillation in patients undergoing isolated coronary artery bypass grafting. Braz J Cardiovasc Surg. 2021;36(2):158-64. Available from: https://doi.org/10.21470/1678-9741-2020-0047.
|
| 21. |
Ahmet Kağan AS, Engin M, Amaç B, Aydın U, Eriş C, Ata Y, et al. Effect of del nido cardioplegia use on kidney injury after coronary bypass operations. Rev Assoc Med Bras. (1992) 2021;67(9):1322-7. Available from: https://doi.org/10.1590/1806-9282.20210642.
|
| 22. |
Mehrabanian MJ, Firoozabadi MD, Hossein S, Tafti A, Khalil S, Nia F, et al. Clinical outcomes and electrolyte balance factors in complex cardiac operations in adults; Del Nido® Versus Custodiol® Cardioplegia Solutions: A randomized controlled clinical trial. Iran Red Crescent Med J. 2018;20(4):64648. Available from: https://doi.org/10.5812/ircmj.64648.
|
| 23. |
Duan L, Hu G huang, Wang E, Zhang C liang, Huang L jin, Duan Y ying. Del Nido versus HTK cardioplegia for myocardial protection during adult complex valve surgery: a retrospective study. BMC Cardiovasc Disord. 2021;21(1):604. Available from: https://doi.org/10.1186/S12872-021-02411-W.
|
| 24. |
Lee C hoon, Kwon Y, Park SJ, Lee JW, Kim JB. Comparison of del Nido and histidine-tryptophan-ketoglutarate cardioplegic solutions in minimally invasive cardiac surgery. J Thorac Cardiovasc Surg. 2020;164(4):e161-e171. Available from: https://doi.org/10.1016/J.JTCVS.2020.11.163.
|
| 25. |
Gunaydin S, Akbay E, Gunertem OE, McCusker K, Kunt AT, Onur MA, et al. Comparative effects of single-dose cardioplegic solutions especially in repeated doses during minimally invasive aortic valve surgery. Innovations (Phila) 2021;16(1):80-9. Available from: https://doi.org/10.1177/1556984520967119.
|
| 26. |
Sanetra K, Gerber W, Shrestha R, Domaradzki W, Krzych Ł, Zembala M, et al. The del Nido versus cold blood cardioplegia in aortic valve replacement: A randomized trial. J Thorac Cardiovasc Surg. 2020;159(6):2275-2283.e1. Available from: https://doi.org/10.1016/J.JTCVS.2019.05.083.
|
| 27. |
Orak Y, Kocarslan A, Boran OF, Acipayam M, Eroglu E, Kirisci M, et al. Comparison of the operative and postoperative effects of del Nido and blood cardioplegia solutions in cardiopulmonary bypass surgery. Braz J Cardiovasc Surg. 2020;35(5):689-96. Available from: https://doi.org/10.21470/1678-9741-2019-0436.
|
| 28. |
Koeckert MS, Smith DE, Vining PF, Ranganath NK, Beaulieu T, Loulmet DF, et al. Del Nido cardioplegia for minimally invasive aortic valve replacement. J Card Surg. 2018;33(2):64–8. Available from: https://doi.org/10.1111/JOCS.13536.
|
| 29. |
Sorabella RA, Akashi H, Yerebakan H, Najjar M, Mannan A, Williams MR, et al. Myocardial protection using del nido cardioplegia solution in adult reoperative aortic valve surgery. J Card Surg. 2014;29(4):445-9. Available from: https://doi.org/10.1111/JOCS.12360.
|
| 30. |
Ross JDW, Newland RF, Hamson RTJ, Rice GD, Baker RA. Del Nido cardioplegia in adult cardiac surgery: analysis of myocardial protection and post-operative high-sensitivity Troponin T. ANZ J Surg 2021;91(10):2192-8. Available from: https://doi.org/10.1111/ANS.17135.
|
| 31. |
Ad N, Holmes SD, Massimiano PS, Rongione AJ, Fornaresio LM, Fitzgerald D. The use of del Nido cardioplegia in adult cardiac surgery: A prospective randomized trial. J Thorac Cardiovasc Surg. 2018;155(3):1011-8. Available from: https://doi.org/10.1016/J.JTCVS.2017.09.146.
|
| 32. |
Kim JS, Jeong JH, Moon SJ, Ahn H, Hwang HY. Sufficient myocardial protection of del Nido cardioplegia regardless of ventricular mass and myocardial ischemic time in adult cardiac surgical patients. J Thorac Dis. 2016;8(8):2004-10. Available from: https://doi.org/10.21037/JTD.2016.06.66.
|
| 33. |
Luo H, Qi X, Shi H, Zhao H, Liu C, Chen H, et al. Single-dose del Nido cardioplegia used in adult minimally invasive valve surgery. J Thorac Dis. 2019;11(6):2373-82. Available from: https://doi.org/10.21037/JTD.2019.05.78.
|
| 34. |
Vistarini N, Laliberté E, Beauchamp P, Bouhout I, Lamarche Y, Cartier R, et al. Del Nido cardioplegia in the setting of minimally invasive aortic valve surgery. Perfusion 2017;32(2):112-7. Available from: https://doi.org/10.1177/0267659116662701.
|
| 35. |
Chen HW, Wang L, Wan LL, Xiao LQ, Chen X. Use of del Nido cardioplegia in acute aortic dissection surgery. Perfusion 2021;36(3):233-8. Available from: https://doi.org/10.1177/0267659120938528.
|
| 36. |
Kavala AA, Turkyilmaz S. Comparison of del Nido Cardioplegia with Blood Cardioplegia in Coronary Artery Bypass Grafting Combined with Mitral Valve Replacement. Braz J Cardiovasc Surg. 2018;33(5):496-504. Available from: https://doi.org/10.21470/1678-9741-2018-0152.
|
| 37. |
Schutz A, Zhang Q, Bertapelle K, Beecher N, Long W, Lee VV, et al. Del Nido cardioplegia in coronary surgery: a propensity-matched analysis. Interact Cardiovasc Thorac Surg. 2020;30(5):699-705. Available from: https://doi.org/10.1093/ICVTS/IVAA010.
|
| 38. |
Shu C, Hong L, Shen X, Zhang W, Niu Y, Song X, et al. Effect of Del Nido cardioplegia on ventricular arrhythmias after cardiovascular surgery. BMC Cardiovasc Disord. 2021;21(1):32. Available from: https://doi.org/10.1186/S12872-020-01844-Z.
|
| 39. |
George G, Varsha A V., Philip MA, Vithayathil R, Srinivasan D, Sneha Princy FX, et al. Myocardial protection in cardiac surgery: Del Nido versus blood cardioplegia. Ann Card Anaesth. 2020;23(4):477-84. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7879885/.
|
| 40. |
Shi H, Luo H, Qi X, Zhao H, Liu C, Chen H, et al. del Nido cardioplegia in surgery for aortic root disease: a historically controlled study. J Thorac Dis. 2020;12(8):4105-14. Available from: https://doi.org/10.21037/JTD-20-1101.
|
| 41. |
Pragliola C, Hassan E, Ismail H, Al Otaibi K, Alfonso JJ, Algarni KD. del Nido cardioplegia in adult patients: a propensity-matched study of 102 consecutive patients. Heart Lung Circ. 2020;29(9):1405-11. Available from: https://doi.org/10.1016/J.HLC.2019.08.019.
|
| 42. |
Ramanathan R, Parrish DW, Armour TK, Brinster DR. Use of del Nido cardioplegia in adult cardiac surgery. Thorac Cardiovasc Surg. 2015;63(7):624-7. Available from: https://doi.org/10.1055/S-0035-1545260.
|
| 43. |
Ali JM, Miles LF, Abu-Omar Y, Galhardo C, Falter F. Global cardioplegia practices: results from the global cardiopulmonary bypass survey. J Extra Corpor Technol. 2018;50(2):83-93. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6002645/.
|
| 44. |
Matte GS, Del Nido PJ. History and Use of del Nido Cardioplegia Solution at Boston Children’s Hospital. J Extra Corpor Technol. 2012;44(3):98-103. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4557532.
|
| 45. |
Govindapillai A, Hua R, Rose R, Friesen CH, O’Blenes SB. Protecting the aged heart during cardiac surgery: Use of del Nido cardioplegia provides superior functional recovery in isolated hearts. J Thorac Cardiovasc Surg. 2013;146(6):940-8. Available from: https://doi.org/10.1016/j.jtcvs.2013.05.032.
|
| 46. |
O’Brien JD, Howlett SE, Burton HJ, O’Blenes SB, Litz DS, Friesen CLH. Pediatric cardioplegia strategy results in enhanced calcium metabolism and lower serum troponin T. Ann Thorac Surg. 2009;87(5):1517-23. Available from: https://doi.org/10.1016/j.athoracsur.2009.02.067.
|
| 47. |
Mick SL, Robich MP, Houghtaling PL, Gillinov AM, Soltesz EG, Johnston DR, et al. del Nido versus buckberg cardioplegia in adult isolated valve surgery. J Thorac Cardiovasc Surg. 2015;149(2):626-636.e5. Available from: https://doi.org/10.1016/J.JTCVS.2014.10.085.
|
| 48. |
Misra S, Srinivasan A, Jena SS, Bellapukonda S. Myocardial protection in adult cardiac surgery with del Nido versus blood cardioplegia: a systematic review and meta-analysis. Heart Lung Circ. 2021;30(5):642-55. Available from: https://doi.org/10.1016/J.HLC.2020.10.016.
|
| 49. |
Ong GS, Guim GS, Lim QX, Chay-Nancy HS, Jaafar NB, Lim CA, et al. Alternative technique of long acting cardioplegia delivery results in less hemodilution. Perfusion 2020;36(4):365-73. Available from: https://doi.org/10.1177/0267659120946727.
|
| 50. |
Yammine M, Neely RC, Loberman D, Rajab TK, Grewal A, McGurk S, et al. The use of lidocaine containing cardioplegia in surgery for adult acquired heart disease. J Card Surg. 2015;30(9):677-84. Available from: https://doi.org/10.1111/JOCS.12597.
|
| 51. |
Sevuk U, Dursun S, Ar ES. Tepid modified del Nido cardioplegia in adults undergoing cardiac surgery: a propensity-matched analysis. Braz J Cardiovasc Surg. 2021; 37(6):793-800. Available from: https://doi.org/10.21470/1678-9741-2020-0422.
|
| 52. |
D’angelo AM, Nemeth S, Wang C, Kossar AP, Takeda K, Takayama H, et al. Re-dosing of del Nido cardioplegia in adult cardiac surgery requiring prolonged aortic cross-clamp. Interact Cardiovasc Thorac Surg. 2022;34(4):556-63. Available from: https://doi.org/10.1093/ICVTS/IVAB310.
|
