

Comparative study on awareness about carpal tunnel syndrome among dental professionals in India and Malaysia


Abstract
Introduction: Carpal Tunnel syndrome (CTS) is a common medical condition that occurs when the median nerve is compressed at the carpal tunnel. Many people, particularly females, in the general population are affected with CTS. This study aims to determine the level of awareness of CTS among dental professionals in India and Malaysia.
Material and Methods: The cross-sectional study was carried out among dentists in India and Malaysian, from August 2020 to November 2020. 150 professional dentists with a minimum of one year of work experience were included in the study. Dentists who worked full-time as academicians were excluded. The survey form was circulated using WhatsApp. The SPSS software package was used to analyze the data collected from the sample.
Results: Both Indian and Malaysian participants thought that the main symptom is tingling and numbness. Both groups stated that minimizing the stress on the wrist would prevent CTS. 100% of Malaysian participants thought that CTS could affect job performance, though those from Indian marked that it also affects social life and sleep.
Conclusion: The awareness of CTS among both Indian and Malaysian dentists was adequate. Furthermore, there is a strong correlation between CTS and chronic disease like rheumatoid arthritis.
Citation
Devi R, Kumar S, Priya A. Comparative study on awareness about carpal tunnel syndrome among dental professionals in India and Malaysia. Eur J Transl Clin Med. 2022;5(2):37-41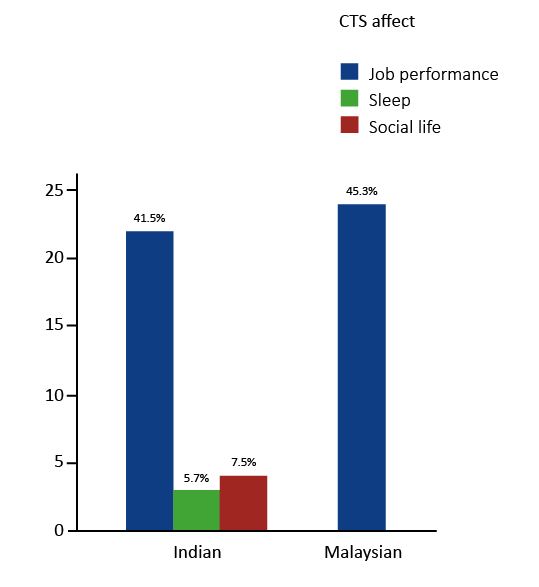







Introduction
Carpal Tunnel syndrome (CTS) is a common medical condition that occurs when the median nerve is compressed at the carpal tunnel [1]. It may also describe radiculopathy or peripheral neuropathy [2]. In CTS, the pressure is increased within the carpal tunnel; therefore it reduces the movement at the level of wrist [3]. The clinical symptoms include burning sensation and paresthesia in digits except the ulnar half of fourth (ring) and fifth (little) fingers [4]. These symptoms are exacerbated at night and in the morning [5]. In order to relieve discomfort or symptoms, patients flick or ‘shake out’ their hand at the level of the wrist (flick sign) [6]. If not treated, CTS may lead to wasting and atrophy of thenar muscles.
Nearly 3.5% of the general population is considered to have CTS [7]. Women are more likely to acquire CTS than men due to hormonal changes [8]. CTS is mostly diagnosed with the age group between 30 and 60 years. According to the literature, we can expect that at least one in every five symptomatic individuals has CTS. The first step in diagnosing CTS is paying attention to the presence of distinctive symptoms in the patient’s history. The physical examination of the patient’s hand is a critical step in the diagnosis of CTS since certain findings may suggest the presence of other causes. The Tinel sign and Phalen manoeuvre are the initial diagnostic procedures for CTS during the physical examination [7, 9-10].
Certain medical conditions increase the risk of developing CTS, e.g. hypothyroidism, arthritis, and high blood pressure [10]. Lifestyle can also increase risk of CTS, e.g. sedentary lifestyle, pregnancy, high salt intake and increase body mass index [11]. Dental professionals are at increased risk of developing CTS due to repetitive hand motions in their clinical practice [12]. CTS is a serious diagnosis for dental professionals, as they rely on full range of motion and sensation in hands in order to perform procedures. Considering the importance of this syndrome and its high incidence among dentists, we aimed to study the level of awareness about CTS among dental professionals in India and Malaysia.
Materials and methods
The cross-sectional study was carried out among dentists in India and Malaysian, from August 2020 to November 2020. 150 professional dentists with a minimum of one year of work experience were included in the study; dentists who worked full-time as academicians were excluded. Ethical Committee approval was obtained from the Saveetha Institute of Medical and Technical Sciences (SIMATS). We prepared a 6-item, multiple-choice questionnaire (see Supplementary Materials) and made it available online until we reached the target sample size. The survey form was circulated through WhatsApp and only those who agreed on the consent form could take up the survey else they cannot proceed further. The IBM SPSS version 23 (Armonk, NY, United States) package was used to analyze the data and calculate the Pearson chi squared test.
Results
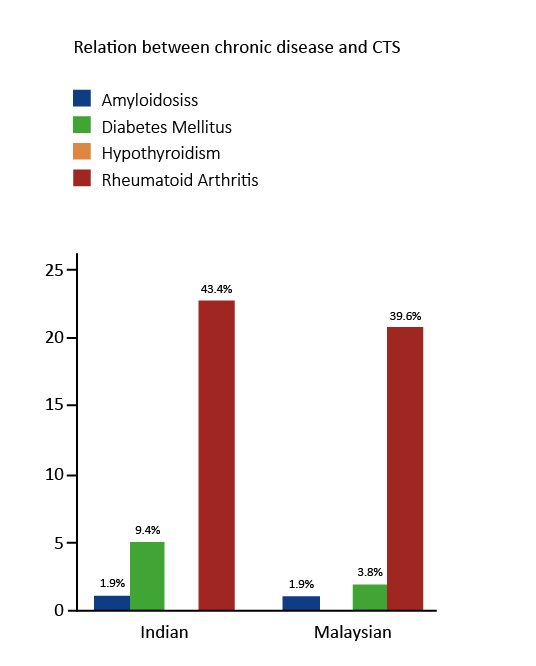
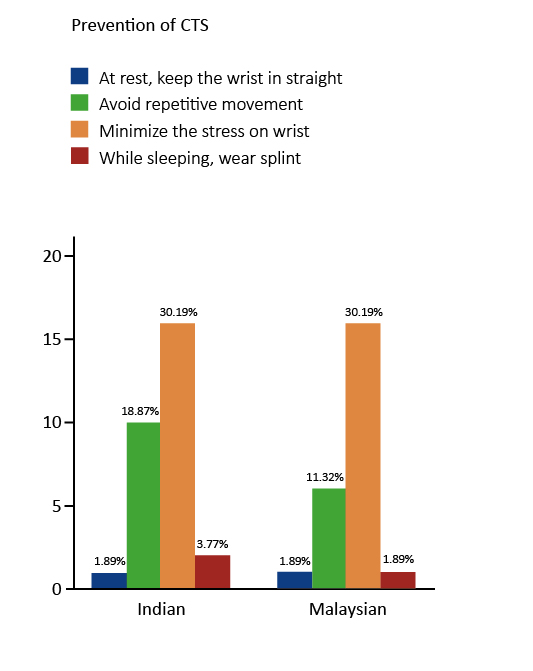
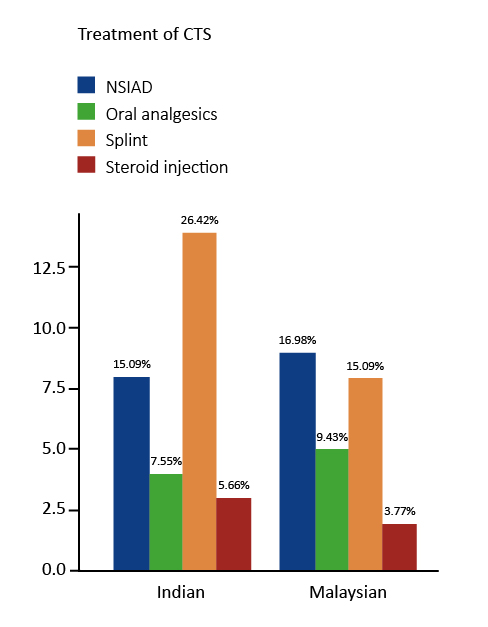
A total of 150 dentists were participated in our study. In the present study, the awareness level of both Indian and Malaysians about CTS is ample. Both Indian and Malaysian participants thought that the main symptom is tingling and numbness. Both populations were suggested that minimizing the stress on the wrist would prevent CTS. 100% of Malaysian participants thought that CTS could affect job performance, though the Indian participants marked that it also affects social life and sleep. Least number of people from both populations believed to wear a splint during sleep to keep wrist in straight would be effective on CTS (Figure 3). 26% of Indians and 15% of Malaysians believed that splint is the one of the main treatments for CTS. 16% of Malaysians and 15% of Indians believed that NISAD is the second-best treatment for CTS. 100% of Malaysian’s thought that CTS affects job concert, but Indians suspected that 75% affect job, 11% sleep and 14% of them felt affecting the social life (Figure 1). Rheumatoid arthritis (RA) people have the higher chance of developing CTS which was thought by Indians and Malaysians. But very few Malaysians believed hypothyroidism too (Figure 2).
Figure 1. Both Indian and Malaysian participants were aware of CTS effect on job performance (p = 0.03)
Figure 2. Indian participants were more aware that people suffering from rheumatoid arthritis have a greater risk of
CTS (p = 0.08)
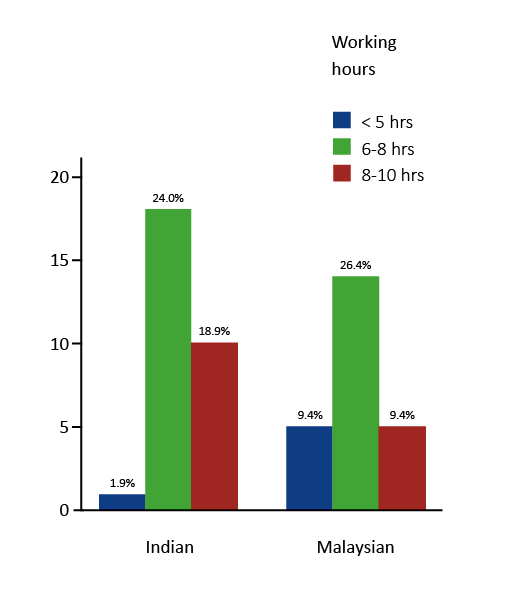
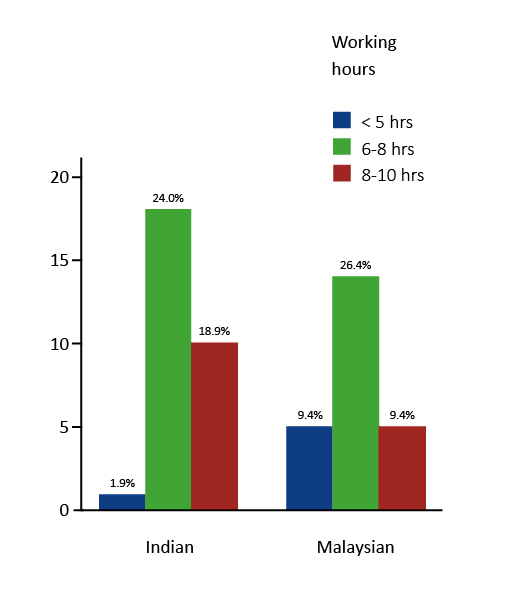
Figure 3. Indian participants stated that they were working for 6-8 hrs more per day than Malaysians (p = 0.11)
Disscussion
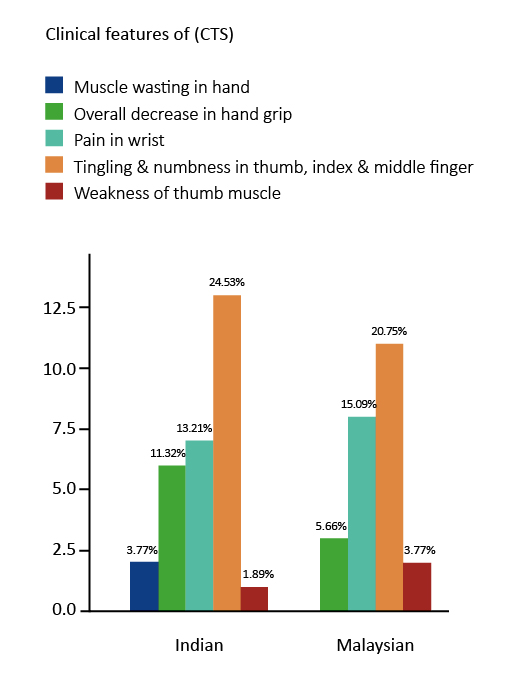
Most of the Indian and Malaysian dentists work for 6-7 hours per day and very few only work less than five hours per day (Figure 3). The more time the dentist spends working, the more chances of occurrence of CTS symptoms. A previous study in the Saudi population showed that increased hand pain and symptoms are evident in those who are working with patients for more than eight hours [12]. In addition, earlier studies revealed that dentists who worked for extensive hours were more likely to develop CTS [13-14]. In our study, both the Indian and Malaysian dentists agreed that tingling and numbness in the thumb, index and middle finger is the main clinical feature of CTS. The second most commonly reported clinical feature reported by both groups was pain in the wrist, then overall decrease of hand grip strength (Figure 4). Haghighat et al determined the CTS based on numbness of fingers [15]. In several studies it was reported that dentists suffering from CTS complained of having severe pain in the hand and wrist [16-17]. In the present study, both Malaysians and Indians were not aware that pain in the wrist is the foremost clinical feature of CTS. In a study by Page et al, more than 10% of participants noted that avoiding repetitive movement also prevents CTS, which is disparate to our present study (Figure 5) [18].
Figure 4. Indian participants were more aware about the clinical features of CTS (p = 0.53)
Figure 5. Indian participants were more aware that avoiding repetitive movement can prevent CTS (p = 0.83)
Wellman et al reported that changing tools and tasks, thus decreasing recurrent wrist movements, were steps to prevent CTS [19]. By increasing the number of breaks, reducing work hours, and decreasing the recurrent wrist movement would prevent the CTS [20]. Alyousef et al revealed that oral analgesics and splint are most used to cure CTS [21]. However in our study, both Indian and Malaysian dentists were not aware that oral analgesics can also be used to treat CTS (Figure 6). Marshal et al reported that steroid injections led to improvement of CTS symptoms but in our study only 3 -5% participants were aware of it [22]. Our results are similar to those reported by Alyousef et al, in which most of the participants agreed that CTS affects their job performance [21, 23]. But Indians are not aware that hypothyroidism people have a risk of emerging CTS.
Figure 6. Malaysian participants were more aware of oral analgesics in the treatment of CTS (p = 0.67)
The main limitation of this study is the low survey response rate, because it was carried out in small group. Second, because this was a pilot study, the inferential statistics may not fully reflect the populations of Indian and Malaysian dentists. More research is needed to confirm the current findings via patient examination (functional and clinical symptoms of CTS). A future study may be carried out among the dentists working in different specialties to find the stage of CTS that pertained to them.
Conclusions
Based on the data, both the community population had an adequate knowledge on CTS among dentists. Furthermore, there is a strong relation between CTS and rheumatoid arthritis. Dentists are more susceptible to CTS, hence they should take extra steps to avoid it. Increased awareness of the threat of CTS among dentists may help to reduce the risk of CTS, resulting in better quality of dental care. The successful management of CTS may be influenced by early detection of symptoms and education about occupational exposure. Early intervention is critical for dentists who are at a higher risk of acquiring CTS or are already experiencing its symptoms.
Acknowledgements
The authors are thankful to all the survey participants for their full cooperation.
Funding
None.
Conflicts of interest
None.
References
| 1. |
Burton C, Chesterton LS, Davenport G. Diagnosing and managing carpal tunnel syndrome in primary care. Br J Gen Pract [Internet]. 2014 May 1;64(622):262–3. Available from: http://bjgp.org/content/64/622/262.abstract.
|
| 2. |
Alfonso C, Jann S, Massa R, Torreggiani A. Diagnosis, treatment and follow-up of the carpal tunnel syndrome: a review. Neurol Sci [Internet]. 2010 Jun 10;31(3):243–52. Available from: https://doi.org/10.1007/s10072-009-0213-9.
|
| 3. |
American Academy of Orthopaedic Surgeons. Clinical Guideline on Diagnosis of Carpal Tunnel Syndrome [Internet]. American Academy of Orthopaedic Surgeons. 2007 [cited 2022 Aug 22]. Available from: https://www.aaos.org/aaosnow/2007/jul/clinical/clinical4/.
|
| 4. |
Braddom RL. Physical Medicine & Rehabilitation. 3rd ed. Philadelphia: Elsevier Saunders; 2007. 1079–80 p.
|
| 5. |
Dorwart BB. Carpal tunnel syndrome: A review. Semin Arthritis Rheum [Internet]. 1984 Nov;14(2):134–40. Available from: https://www.sciencedirect.com/science/article/pii/0049017284900039.
|
| 6. |
Krendel DA, Jobsis M, Gaskell PC, Sanders DB. The flick sign in carpal tunnel syndrome. J Neurol Neurosurg Psychiatry [Internet]. 1986 Feb 1;49(2):220–1. Available from: http://www.ncbi.nlm.nih.gov/pubmed/3950646.
|
| 7. |
Atroshi I, Gummesson C, Johnsson R, Ornstein E, Ranstam J, Rosén I. Prevalence of Carpal Tunnel Syndrome in a General Population. JAMA [Internet]. 1999 Jul 14;282(2):153–8. Available from: https://doi.org/10.1001/jama.282.2.153.
|
| 8. |
Phalen G. The carpal-tunnel syndrome. J Bone Jt Surg Am. 1966;48(A):380–3.
|
| 9. |
Phalen G. The carpal tunnel syndrome; seventeen years’ experience in diagnosis and treatment of six hundred fifty-four hands. J Bone Jt Surg. 1966;48(A):211–28.
|
| 10. |
De Krom MCTFM, Knipschild PG, Kester ADM, Thijs CT, Boekkooi PF, Spaans F. Carpal tunnel syndrome: Prevalence in the general population. J Clin Epidemiol [Internet]. 1992;45(4):373–6. Available from: https://www.sciencedirect.com/science/article/pii/089543569290038O.
|
| 11. |
Becker J, Nora DB, Gomes I, Stringari FF, Seitensus R, Panosso JS, et al. An evaluation of gender, obesity, age and diabetes mellitus as risk factors for carpal tunnel syndrome. Clin Neurophysiol [Internet]. 2002;113(9):1429–34. Available from: https://www.sciencedirect.com/science/article/pii/S1388245702002018.
|
| 12. |
Ahmed AF, Mashael A, Fadwa A, Alanoud A, Bassam A, Emad M, et al. Prevalence of carpal tunnel syndrome symptoms among dentists working in Riyadh. Ann Saudi Med [Internet]. 2019 Mar 1;39(2):104–11. Available from: https://doi.org/10.5144/0256-4947.2019.07.03.1405.
|
| 13. |
Leggat PA, Smith DR. Musculoskeletal disorders self-reported by dentists in Queensland, Australia. Aust Dent J [Internet]. 2006 Dec 1;51(4):324–7. Available from: https://doi.org/10.1111/j.1834-7819.2006.tb00451.x.
|
| 14. |
Palmer KT. Carpal tunnel syndrome: The role of occupational factors. Best Pract Res Clin Rheumatol [Internet]. 2011;25(1):15–29. Available from: https://www.sciencedirect.com/science/article/pii/S1521694211000192.
|
| 15. |
Haghighat A, Khosrawi S, Kelishadi A, Sajadieh S, Badrian H. Prevalence of clinical findings of carpal tunnel syndrome in Isfahanian dentists. Adv Biomed Res [Internet]. 2012;1:13. Available from: http://www.ncbi.nlm.nih.gov/pubmed/23210072.
|
| 16. |
Alexopoulos EC, Stathi I-C, Charizani F. Prevalence of musculoskeletal disorders in dentists. BMC Musculoskelet Disord [Internet]. 2004;5(1):16. Available from: https://doi.org/10.1186/1471-2474-5-16.
|
| 17. |
Leggat PA, Kedjarune U, Smith DR. Occupational Health Problems in Modern Dentistry: A Review. Ind Health [Internet]. 2007;45(5):611–21. Available from: https://www.jstage.jst.go.jp/article/indhealth/45/5/45_5_611/_article.
|
| 18. |
Page MJ, O’Connor D, Pitt V, Massy‐Westropp N. Exercise and mobilisation interventions for carpal tunnel syndrome. Cochrane Database Syst Rev [Internet]. 2012;(6). Available from: https://doi.org//10.1002/14651858.CD009899.
|
| 19. |
Wellman H, Davis L, Punnett L, Dewey R. Work-related carpal tunnel syndrome (WR-CTS) in Massachusetts, 1992–1997: Source of WR-CTS, outcomes, and employer intervention practices. Am J Ind Med [Internet]. 2004 Feb 1;45(2):139–52. Available from: https://doi.org/10.1002/ajim.10326.
|
| 20. |
Žídková V, Nakládalová M, Zapletalová J, Nakládal Z, Kollárová H. Experiences with preventing carpal tunnel syndrome in an automotive plant. Int J Occup Med Environ Health [Internet]. 2017;30(1):45–54. Available from: https://doi.org/10.13075/ijomeh.1896.00793.
|
| 21. |
Alyousef YY, Alyousef FY, Almaymoni SM, Hazizi M, Almaymoni MM, Alyousef AY, et al. Awareness of carpal tunnel syndrome among adult population of Al Majmaah city, Saudi Arabia, 2018–2019. J Fam Med Prim Care [Internet]. 2019;8(10):3383. Available from: https://journals.lww.com/10.4103/jfmpc.jfmpc_400_18.
|
| 22. |
Braun RM, Davidson K, Doehr S. Provocative testing in the diagnosis of dynamic carpal tunnel syndrome. J Hand Surg Am [Internet]. 1989;14(2, Part 1):195–7. Available from: https://www.sciencedirect.com/science/article/pii/0363502389900051.
|
| 23. |
Stevens JC, Beard CM, O’Fallon WM, Kurland LT. Conditions Associated With Carpal Tunnel Syndrome. Mayo Clin Proc [Internet]. 1992;67(6):541–8. Available from: https://www.sciencedirect.com/science/article/pii/S0025619612604613.
|
