

Do parents properly assess children’s physical activity level? Study of over 20 thousand children and parents dyads


Abstract
Background
From the public health perspective, it is particularly important to establish links between a persons' perception of their own health and their predispositions to undertake pro-health behaviours that enable them to maintain proper functioning of their body. In the case of the paediatric population, it is crucial to emphasise that adults are responsible for the adoption and development of appropriate health-enhancing behaviours by children. The aim of this study is to verify parents' perception of the level of children’s physical activity (PA) in comparison with objective measures describing children's physical fitness.
Material and methods
Material for analysis consists of the results of anthropometric tests and cardiopulmonary exercise capacity of children as well as questionnaires concerning 28,891 children completed by parents.
Results
In more than 40% of the sample, the subjectively assessed level of PA was not consistent with the cardiorespiratory fitness level. It was observed that the correct assessment of the level of PA of children is more common for girls, increases with the age of the child and with the level of parental education.
Citation
Metelska P, Brzeziński M, Jankowski M, Niedzielska A, Szarszewski A. Do parents properly assess children’s physical activity level? Study of over 20 thousand children and parents dyads. Eur J Transl Clin Med. 2021;4(2):52-59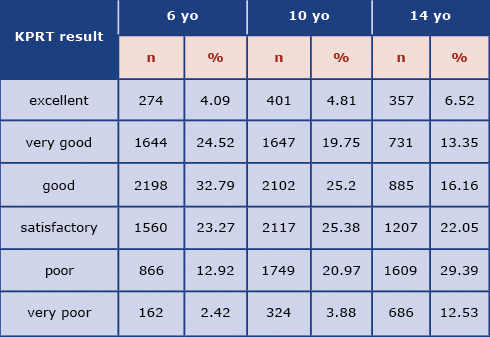










Introduction
Over the last few decades, significant changes related to the level of physical activity among adults and children took place in most of developed societies. About 30 years ago in Poland, after the collapse of the communist government, the socio-economic conditions of the citizens significantly improved. Easier access to high-energy food and lifestyle changes were observed [1]. For several different reasons (e.g. safety, distance, time) the broadly understood mobility patterns have changed, with walking giving way to driving and using public transport, both of which reduce energy expenditure on daily basis [2]. Physical activity limited to the school environment alone does not allow the child to have the minimum recommended amount of daily exercise [3]. These changes also relate to children and young people spending more time in front of the television or computer, which is one of the risk factors for the decreasing physical activity level [4].
Health Behaviour In School-Aged Children (HBSC) research carried out between 2002 and 2010 in more than 30 countries showed that 77% of boys and 86% of girls in the countries included in the study are at risk of ill health due to insufficient physical activity [5]. The results of the Polish edition of the WHO (World Health Organisation) European Childhood Obesity Surveillance Initiative (COSI) study indicate that for more than half of 8-year-olds their journey to school does not involve any physical activity. At the same time, the authors report that parents declared in the survey that 82.9% of children followed the WHO recommendations and accumulated 60 minutes or more physical activity during the school day [6]. From the practical perspective, it is particularly important to establish links between person's perception of their own health and their predispositions to undertake pro-health behaviors that enable them to maintain best available health status [7]. In the case of the pediatric population, it is crucial to emphasize that adults are responsible for the adoption and development of appropriate health-enhancing behaviors by children and adolescents [7].
Interviewing parents/guardians either via a personal conversation or using surveys on health status and health behavior is the basis for a system of health statistics in all European countries [7]. It is generally accepted that survey responses are provided by parents/legal guardians who make the assessment. Therefore the data concerning health assessment of children are provided from the perspective of their parents and/or guardians [8]. Proper assessment by parents is often essential to ensure that they take appropriate and necessary measures to maintain the health of their child. However, questions arise as to the objectivity of such an assessment.
The aim of this study is to verify parents' perception of the level of children’s physical activity in comparison with objective measures describing children's physical fitness. The analysis reported in this article was carried out within the scope of a population-based health program "6-10-14 for Health" designed to manage and reduce the risk factors of civilization diseases in children and adolescents, carried out by the University Clinical Centre in Gdańsk and funded by the Gdańsk City Hall since 2011.
Materials and Methods
Material for analysis consists of the results of anthropometric tests and cardiopulmonary exercise capacity of children as well as 28,891 questionnaires completed by parents/legal guardians concerning children and adolescents between 6 and 14 years of age from the City of Gdańsk. The results were obtained between 05/09/2011 and 14/02/2017 from children and parents participating in screening tests carried out within the "6-10-14 for Health" program [9]. The sample population represents over 65% of all population of all the children available for screening living in Gdansk aged 6, 9-11, 14 in the years 2011-2017. As the program “6-10- 14 for Health” is designed to screen all children from the City of Gdańsk at the above-mentioned intervals and invites children with overweight and obesity to a one-year-long lifestyle modification intervention. In this article we present the data we obtained only from the screening.
The analysis included only the fully completed questionnaires from the parents of children who underwent full screening (Supplementary material). The parents chose the suggested answers, which in their opinion best described their child’s situation. The respondents were also asked to provide estimates of each parent’s body weight, height and to indicate highest education level.
The assessment of cardiorespiratory fitness (physical capacity) was performed using the Kasch Pulse Recovery Test (KPRT), a simple 3-minute step test that assesses the cardiorespiratory fitness of an individual based on changes in pulse within the first minute after performing the test [10]. The results were compared to dedicated reference systems [10]. The interpretation and evaluation of the responses to the questionnaires was based on the current WHO guidelines for physical activity [11], which indicate that a minimum of 60 minutes of physical activity each day is necessary for a child's normal development, ideally an aerobic effort of medium to moderate intensity.
Our study was conducted with the approval of an independent bioethics committee at the Medical University of Gdańsk (NKBBN/228/2012), in accordance with the requirements of the Helsinki Declaration. Each parent/legal guardian had to express written consent to the child's participation in the program. 6-10-14 for Health program is retrospectively registered in clinical trials database: clinicaltrials.gov no. NCT04143074
Normality of quantitative variables was assessed using the Shapiro-Wilk test, and descriptive statistics included were presented as arithmetic means and upper and lower limits of the 95% confidence interval for the mean (95% CI). Mann-Whitney U test and Kruskal-Wallis test with Dunn's post-hoc test were used for between-groups comparisons of quantitative variables. The strength and direction of the relationship between pairs of quantitative variables were evaluated on the basis of the Spearman's Rank Correlation Factor (R). Pearson's chi-quadrant test was used for between-groups comparisons of distributions of qualitative variables. All calculations were performed using Statistica 10 software (StatSoft, United States), with the value of p≤0.05 as the threshold of statistical significance. The effects of variables, which turned out to differ significantly between the compared groups, were evaluated using one- and multi-dimensional logistic regression analysis.
Results
The analysis of the results carried out for the purposes of this study includes the results of objective and subjective assessments, as well as objectivization of subjective assessments. 18% of the questionnaires were rejected due to incompleteness. The study took into account results from of 24981 children aged 6, 9-11 (for the sake of simplicity, in the results we labeled this group the term “10 years old”) and 14 years old. Physical fitness of children was assessed using the Kasch Pulse Recovery Test (KPRT) method, with 20519 children (82.14% of the sample) taking part in t he test. A detailed distribution of Kasch Pulse Recovery Test results by age group is presented in Table 1.
Table 1. KPRT results by age
The group of 10-year-olds was the most numerous and constituted 42.25% of the sample. 6-year-olds and 14-yearolds constituted 33.39% and 24.36%, respectively. Girls and boys constituted respectively 50.03% and 49.97% of the studied group, sex distribution in the sample is presented in Table 2.
Table 2. KPRT results by sex
The studies of cardiopulmonary efficiency show that low (poor and very poor) cardiopulmonary efficiency is similarly common in boys and girls. The analysis did not reveal any significant differences between groups (Pearson's chi- squared test, p = 0.098) and percentage of children with poor and very poor cardiorespiratory (Pearson's square chi test, p < 0.001).
Regarding the physical activity status, 73.79% of parents indicated that in their opinion the child had enough exercise during the day, while 20.71% of parents noticed deficiencies in this area and 5.5% responded "I don't know.”
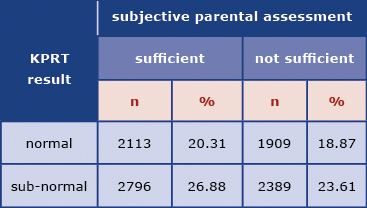
In order to facilitate the comparison of KPRT results with the parental subjective assessment of their children’s activity levels, the KPRT results were re-classified as either “normal fitness” (evaluation of cardiopulmonary efficiency: excellent, very good and good) or “abnormal fitness” (evaluation of cardiopulmonary efficiency: satisfactory, poor and very poor) [10]. The comparison demonstrated that the subjective assessments were not very consistent with the fitness evaluation based on the KPRT (Kendall's Tau-b coefficient = 0.170). In more than 40% of the sample, the subjectively assessed level of physical activity was not consistent with the cardiorespiratory fitness level measured by KPRT, with 33.67% of children assessed as having enough exercise yet performing sub-normally on KPRT and another 9% of the children performing normally despite their parents assessing their activity level as insufficient. It was observed that in 33.67% of the children the level of physical activity considered by their parents as sufficient did not translate into a normal result of the cardiopulmonary efficiency test as presented in Table 3.
Table 3. Consistency of the assessment of cardiopulmonary efficiency of the examined children with the level of their physical activity subjectively assessed by the parent
In order to assess the physical fitness and behaviors related to physical activity of children and adolescents, two additional questions about physical activity-related behavior were included in the questionnaire for parents/guardians.
In response to a question about screen time, 15.59% of parents estimated the time spent by their children in front of a screen as < 1 hour a day, 54.8% of parents indicated that their child spent 1-3 hours in front of a screen and 29.61% of parents indicated that screen time exceeded 3 hours a day.
The second question concerned the number of hours spent by the child on physical activity during the week. Parents responded as follows: minimum 5 hours (31.14%), 3-5 hours (27.09%), 1-3 hours (31.51%), < 1 hour (10.26%).
Based on the WHO recommendations [11] on physical activity of children and adolescents, the parents’/guardians’ responses parents were classified into two categories indicating that the child has or has not developed desirable physical activity behaviors. In order for the behavior to qualify as desirable, parents/legal guardians had to indicate that the child spends <1 hour in front of a television/computer per day and that the child spends at least 5 hours per week actively playing/doing sport (excluding PE classes). Any other answer to either of the questions led to classifying the child into a group with undesirable behaviors. This is how the category of objectivized parental assessment was created. Desirable behavior was demonstrated in 5.72% of children. The remaining answers fell in the category of undesirable behaviors.
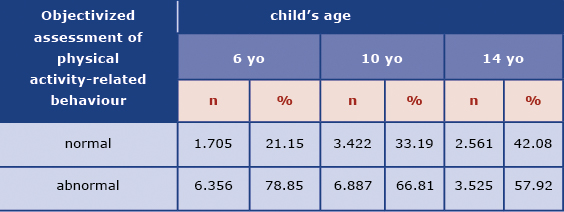
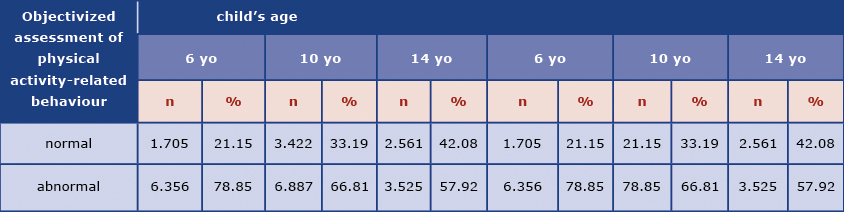
This objectivized assessment of physical activity behavior was compared with the assessment of the KPRT results as shown in Table 4.
Table 4. Assessment of cardiopulmonary efficiency in the examined children versus the objectivized assessment of physical activity-related behaviours
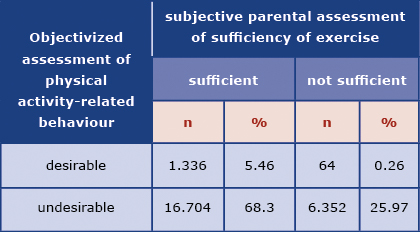
Based on objectivizing the parents’/guardians’ answers to the relevant question, sub-normal results in cardiorespiratory fitness test were observed more frequently among children categorised as having undesirable physical activity patterns (Pearson's chi-quadrant test, p < 0.001). The objectivized assessment of physical activity-related behavior was also compared with the parents' answer to the question "In your opinion, does your child have enough exercise during the day?” as shown in Table 5.
Table 5. Comparison of the child's physical activity subjectively assessed by the parent with the objectivized assessment of physical activity-related behaviours
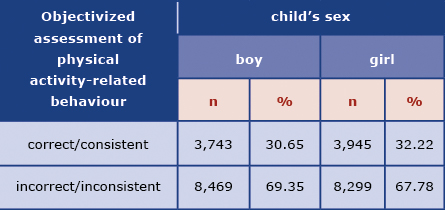
It was analysed whether the child's age, sex or parental education level influenced the consistency of the subjective assessment with behavioral estimates. It was observed that the correct assessment of the level of physical activity of children is more common for girls (Table 6), increases with the age of the child (Table 7) and with the level of parental education (Table 8).
Table 6. Parental assessments of sufficient amount of exercise versus the objectivized physical-activity-related behaviour by sex
Table 7. Parental assessments of sufficient amount of exercise versus the objectivized physical-activity-related behaviour by age
Table 8. Parental assessments of sufficient amount of exercise versus the objectivized physical-activity-related behaviour by parental education
More consistent assessments were observed among parents of girls than among parents of boys (Pearson's chi-quadratic test, p = 0.008).
Discussion
The participation of parents/legal guardians can be observed at different stages in the diagnostic processes of children and adolescents, starting with the consent to perform tests, providing information necessary to interpret the results, to making the diagnosis and planning the appropriate course of action. The parents' knowledge of health behaviors and factors influencing their child's health is an invaluable addition to the physical examination [12]. It should be noted, however, that there are several factors that may distort or falsify information about the health condition of the child, e.g.:
- parents' misunderstanding of the behavior typical for a given phase of a child’s development;
- incompatibility between parental expectations and the child’s characteristics;
- parental characteristics (e.g. depression, lack of interest in the child, rejection, overprotection);
- stress (resulting from family or material situation, etc.) [13].
A reliable assessment of physical activity levels in children and adolescents is a key element of health assessment. It is also the starting point for therapeutic recommendations from specialists and their implementation by children and adolescents under the supervision of their parents/legal guardians. This article presents an attempt to evaluate the reliability of assessments made by parents/guardians, comparing them with objective and objectivized measures. The reliability and accuracy of the assessments was verified on the basis of objective test results but also by asking parents questions that verified or providing more details concerning the areas of interest. The child’s or parent's characteristics that influenced parental assessments were also identified.
The study showed that making a correct assessment of lifestyle-related behaviors is difficult for parents. It was observed that in 33.67% of children the level of physical activity considered by their parents as sufficient did not translate into the normal result of the cardiopulmonary efficiency test. Moreover, 68.30% of parents positively assessed their child’s level of activity although their reported actual level of physical activity was less than desirable. Similar results can be found in British studies, where 80% of parents of inactive children wrongly assessed their children as sufficiently active [14]. Another British study showed that parents perceived physical activity itself as beneficial, but did not have knowledge about the recommendations, and assumed that organizing physical activity for children is primarily the responsibility of the school [15].
The parents' perspective may also be distorted by the emotional context. A study comparing evaluations of parents’ own physical activity during their childhood with the current activity of their children showed that parents perceived their own activity as free and joyful. Despite this positive image, because of their concern for their children's safety, parents limit their children’s free play outdoors. Some parents see the opportunities for structured physical activity in children participating in group activities, but perceive them as a "less joyful" than the free play they recall from their own childhood [16]. Concerns about child safety, lack of financial resources and difficulties in motivating children to engage in physical activity are the most common barriers to introducing physical activity reported by parents [15].
Correct assessment of the level of physical activity in children is more common for girls and increases with the age of the child and with the level of parental education. Our study indirectly revealed a deficit in the correct understanding of the levels of physical activity recommended for children and adolescents. These results also demonstrate that specialists taking history on physical activity cannot limit their investigation to asking simple questions: additional verification questions are necessary or, if possible, objective tests should be carried out.
In the recent decades, physical fitness of both adolescents and adults has deteriorated, which is demonstrated by the results of the CINDI project (Countrywide Integrated Noncommunicable Disease Intervention) carried out in several European countries within the framework of WHO activities. This is particularly worrying because these recommendations of global experts are not new and should have long become a part of the general public’s awareness. In 2005, a team of experts from the American Heart Association developed a position, subsequently endorsed by the American Academy of Pediatrics, that each child should devote a minimum of 60 minutes a day to moderate to high-intensity motor activity [17]. The research reported in this paper did not assess knowledge in this area. Rather, it aimed to diagnose the current situation and assess the correctness of the parents’ assessments in this area.
Moreover, the analysis of the results of the cardiorespiratory fitness test shows that poor fitness affects more boys than girls and that the percentage of children with poor and very poor fitness increases with age. This is also reflected in many studies conducted in Poland and abroad, which indicate that with age, adolescents become less active due to a greater number of mainly sedentary, activities, both at school and during leisure [18-21]. Restrictions in physical activity of children and young people do not result only from the progressing urbanization and automation, but mainly from the high attractiveness of media and internet content. Moreover, parents’ low physical activity translates into lower physical activity in their children. Research indicates that children and adolescents who perceive their parents as physically active are more often active than their peers who do not have such a parental example [22].
Conclusions
Parental assessments of lifestyle-related behaviors show very low sensitivity and specificity. The results obtained make it possible to question the reliability of data obtained only through questionnaires without using any additional questions or an objective method. All collected data should be assessed with great care as it is based on the parental perceptions. This conclusion should also be reflected in practice: when planning programs to promote healthy lifestyles, there is a need to objectivize parental opinions through the use of verification methods (e.g. verification questions or, if possible, the use of objective measurement tools).
Supplementary material
→ Questionnaire completed by parents/guardians
Conflicts of Interest
The authors declare no conflicts of interest.
References
| 1. |
Physical Activity Factsheets For The 28 European Union Member States Of The Who European Region. (2018). 2020.
|
| 2. |
Walton D, Sunseri S. Factors Influencing the Decision to Drive or Walk Short Distances to Public Transport Facilities. Int J Sustain Transp [Internet]. 2010 Jul;4(4):212–26. Available from: http://www.tandfonline.com/doi/abs/10.1080/15568310902927040.
|
| 3. |
Proctor MH, Moore LL, Gao D, Cupples LA, Bradlee ML, Hood MY, et al. Television viewing and change in body fat from preschool to early adolescence: The Framingham Children’s Study. Int J Obes [Internet]. 2003 Jul 24;27(7):827–33. Available from: http://www.nature.com/articles/0802294.
|
| 4. |
Saelens BE, Sallis JF, Nader PR, Broyles SL, Berry CC, Taras HL. Home Environmental Influences on Children’s Television Watching from Early to Middle Childhood. J Dev Behav Pediatr [Internet]. 2002;23(3):127–32. Available from: https://journals.lww.com/jrnldbp/Fulltext/2002/06000/Home_Environmental_Influences_on_Children_s.1.aspx.
|
| 5. |
Kalman M, Inchley J, Sigmundova D, Iannotti RJ, Tynjala JA, Hamrik Z, et al. Secular trends in moderate-to-vigorous physical activity in 32 countries from 2002 to 2010: a cross-national perspective. Eur J Public Health [Internet]. 2015 Apr 1;25(suppl 2):37–40. Available from: https://academic.oup.com/eurpub/article-lookup/doi/10.1093/eurpub/ckv024.
|
| 6. |
Fijałkowska A, Oblacińska A, Stalmach M. Nadwaga i otyłość u polskich 8-latków w świetle uwarunkowań biologicznych, behawioralnych i społecznych. Raport z międzynarodowych badań WHO European Childhood Obesity Surveillance Initiative (COSI). 2017.
|
| 7. |
Turnock BJ. Public health: what it is and how it works. Jones and Bartlett Learning; 2009. 534 p.
|
| 8. |
Moser A, Korstjens I. Series: Practical guidance to qualitative research. Part 3: Sampling, data collection and analysis. Eur J Gen Pract [Internet]. 2018 Jan 1;24(1):9–18. Available from: https://www.tandfonline.com/doi/full/10.1080/13814788.2017.1375091.
|
| 9. |
Brzeziński M, Jankowski M, Niedzielska A, Danielewicz A, Czarnecka P. Health program “6-10-14 for Health” as an example of comprehensive environmental activities in the field of children obesity. Study protocol and primary results. Appetite [Internet]. 2014 May;76:202. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0195666314000373.
|
| 10. |
Jankowski M, Niedzielska A, Brzezinski M, Drabik J. Cardiorespiratory Fitness in Children: A Simple Screening Test for Population Studies. Pediatr Cardiol [Internet]. 2015 Jan 29;36(1):27–32. Available from: http://link.springer.com/10.1007/s00246-014-0960-0.
|
| 11. |
WHO. Global Recommendations on Physical Activity for Health [Internet]. Global Recommendations on Physical Activity for Health. World Health Organization; 2010. Available from: https://apps.who.int/iris/bitstream/handle/10665/44399/9789245599975_chi.pdf.
|
| 12. |
Ingram S. Taking a comprehensive health history: learning through practice and reflection. Br J Nurs [Internet]. 2017 Oct 12;26(18):1033–7. Available from: http://www.magonlinelibrary.com/doi/10.12968/bjon.2017.26.18.1033.
|
| 13. |
Marcdante KJ, Kliegman R. Nelson essentials of pediatrics [Internet]. Elsevier Health Sciences; 2014. 832 p. Available from: https://books.google.pl/books?hl=pl&lr=&id=hsY0AwAAQBAJ&oi=fnd&pg=PP1&dq=Marcdante+KJ,+Kliegman+R.+Nelson+essentials+of+pediatrics.+832+p.+&ots=fPAEjSaWXh&sig=IeIOh2uzj0N3cOw8fL0iIgm6iok&redir_esc=y#v=onepage&q&f=false.
|
| 14. |
Corder K, van Sluijs EMF, McMinn AM, Ekelund U, Cassidy A, Griffin SJ. Perception Versus Reality. Am J Prev Med [Internet]. 2010 Jan;38(1):1–8. Available from: https://linkinghub.elsevier.com/retrieve/pii/S074937970900628X.
|
| 15. |
Trigwell J, Murphy RC, Cable NT, Stratton G, Watson PM. Parental views of children’s physical activity: a qualitative study with parents from multi-ethnic backgrounds living in England. BMC Public Health [Internet]. 2015 Dec 2;15(1):1005. Available from: http://bmcpublichealth.biomedcentral.com/articles/10.1186/s12889-015-2351-8.
|
| 16. |
Solomon-Moore E, Emm-Collison LG, Sebire SJ, Toumpakari Z, Thompson JL, Lawlor DA, et al. “In my day…”- Parents’ Views on Children’s Physical Activity and Screen Viewing in Relation to Their Own Childhood. Int J Environ Res Public Health [Internet]. 2018 Nov 13;15(11):2547. Available from: http://www.mdpi.com/1660-4601/15/11/2547.
|
| 17. |
Fletcher GF, Balady G, Blair SN, Blumenthal J, Caspersen C, Chaitman B, et al. Statement on Exercise: Benefits and Recommendations for Physical Activity Programs for All Americans. Circulation [Internet]. 1996 Aug 15;94(4):857–62. Available from: https://www.ahajournals.org/doi/10.1161/01.CIR.94.4.857.
|
| 18. |
Baker BL, Birch LL, Trost SG, Davison KK. Advanced Pubertal Status at Age 11 and Lower Physical Activity in Adolescent Girls. J Pediatr [Internet]. 2007 Nov;151(5):488–93. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0022347607003599.
|
| 19. |
Eaton DK, Kann L, Kinchen S, Shanklin S, Flint KH, Hawkins J, et al. Youth Risk Behavior Surveillance — United States, 2011. Morb Mortal Wkly Rep [Internet]. 2012;61(4):1–162. Available from: https://www.cdc.gov/mmWr/preview/mmwrhtml/ss6104a1.htm.
|
| 20. |
Trost SG, Pate RR, Sallis JF, Freedson PS, Taylor WC, Dowda M, et al. Age and gender differences in objectively measured physical activity in youth. Med Sci Sports Exerc [Internet]. 2002 Feb;34(2):350–5. Available from: http://journals.lww.com/00005768-200202000-00025.
|
| 21. |
van Mechelen W, Twisk JW, Post GB, Snel J, Kemper HC. Physical activity of young people: the Amsterdam Longitudinal Growth and Health Study. Med Sci Sports Exerc [Internet]. 2000 Sep;32(9):1610–6. Available from: http://www.ncbi.nlm.nih.gov/pubmed/10994913.
|
| 22. |
Sánchez-Zamorano LM, Solano-González M, Macias-Morales N, Flores-Sánchez G, Galván-Portillo M V, Lazcano-Ponce EC. Perception of parents’ physical activity as a positive model on physical activity of adolescents. Prev Med (Baltim) [Internet]. 2019 Oct;127:105797. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0091743519302737.
|
