

The effectiveness of screening for major cardiovascular risk factors in the population of small towns in Poland


Abstract
Background
Screening represents an important tool to improve detection of cardiovascular risk factors. Uniform standards for screening programs and for evaluation of their effectiveness are still lacking.
Material and methods
The results of the Polish 400 Cities Project (P400CP) were analyzed by age and gender, and with regard to the prevalence and awareness of cardiovascular risk factors. The P400CP population were volunteers reporting for screening tests in small towns, and a representative sample was used as control.
Results
Mean age in the screening group was 10 years more than in the representative sample. Two thirds of participants were women. First-time diagnosis rates for elevated arterial blood pressure, hyperglycemia and hypercholesterolemia in the screening were 28%, 15% and 51%, respectively. Almost 40% of participants reported previously diagnosed hypertension (vs. 25% of the control sample), 7% vs. 4% reported diabetes and 16% vs. 9% – hypercholesterolemia. Smokers represented 16.5% of participants (36% of the control sample).
Conclusions
“Open” screening programs fail in targeting young adults, especially males, and people reporting for screening are often already diagnosed with arterial hypertension and/or diabetes. Despite these limitations, “open” screening is effective in detecting undiagnosed cases of hypercholesterolemia. Non-smokers report for screening tests more often.
Citation
Rutkowski M, Wierucki Ł, Wojciechowska A, Zdrojewski T. The effectiveness of screening for major cardiovascular risk factors in the population of small towns in Poland. Eur J Transl Clin Med. 2021;4(1):57-64







Introduction
Over the past dozen years or so, a decrease in cardiovascular mortality was recorded in Poland. However, cardiovascular diseases still remain the main cause of mortality, including premature mortality, especially among males [1-4]. The results of epidemiology studies indicate several concurrent reasons for this situation: wide prevalence and low detection rates of cardiovascular risk factors and also a disparity between highly-urbanized regions and small-town or rural communities in Poland [5-6]. Therefore, regional and/or national prevention programs have been launched, with screening for cardiovascular risk factors as their main component [7-10]. Polish recommendations (based to a large extent on European guidelines) define criteria such as scope, frequency and target group, but they do not determine all the aspects of screening programs [11-13]. In 2003-2008, under the National POLKARD Program, the Polish 400 Cities Project (P400CP) was carried out, including a screening study [9, 14].
The objective of this article is to provide an assessment to what extent screening programs targeting adult residents of small towns in Poland may be effective in improving the detection of cardiovascular risk factors. To attain this objective, the results of the P400CP were analyzed, including the age and gender structure as well as the prevalence and awareness of selected cardiovascular risk factors. These analyses were carried out both for the population of volunteers reporting for screening tests and for the control sample (a sample representative for the population of small towns).
Methods
Design and execution of the screening study
The P400CP activities were carried out in 319 towns with population below 8000 residents. The project was preceded by an extensive information campaign. Because of the project design (including extensive educational activities and a promotional campaign), and because Poland is lacking an established standard concerning the manner in which people are recruited for screening, a decision was made to take an “open” approach, whereby any adult visiting a medical center could volunteer to participate in screening. The information campaign was based on articles published in the press and online (town council websites), broadcasts on local radio and television, posters and leaflets [9, 14]. Moreover, every household received information in the mail [9, 14]. The materials promoting the program emphasized that screening was targeted to those who had not been diagnosed with the disorders before, and the campaign carried a message about men being the group specifically at risk of prematurely developing cardiovascular conditions. Consequently, men should take particular care to have any risk factors detected early.
The screening took place at established medical centers/local outpatient clinics and was carried out by trained nurses. Over five consecutive days the following tests were performed: a questionnaire interview, anthropometric measurements, two arterial blood pressure readings and strip tests for blood glucose and blood cholesterol. In the afternoons, additional blood pressure readings were taken from those with newly detected elevated values.
The representative survey
The sample in the representative survey included 1278 men and women, aged 19-75, who lived in 85 towns randomly selected out of the pool of 319 towns included in the P400CP screening project. In order to ensure a representative group of subjects, both male and female, within the age range of 19-75 years, a two-tiered sample selection process was applied. Stratified and proportional sampling procedure was used. Territorial layers in all the 16 provinces (województwa) were created, where two classes of towns were specified: towns below 4000 residents and towns with 4000-8000 residents. Each territorial layer was then divided into demographic strata – four age categories for women and men aged 19-30, 31-45, 46-60, and 61-75 years. The number of interviews carried out in each demographic stratum was proportional to the size of the population represented by that stratum in its territorial layer. Individual respondents were drawn by the Ministry of Internal Affairs and Administration. The sampling frame was the central PESEL database (National Electronic System of Population Records).
The representative survey was carried out before the start of the information campaign for the project. Blood pressure readings were taken in a manner identical to that used later in the screening. Blood pressure was measured during two separate visits. The results were analyzed using the outcomes of two readings taken during the first visit, the same as in the screening. In the questionnaire interview, responses to a specific group of questions provided the data for analysis regarding risk factor awareness. No cholesterol or blood glucose readings were taken in the representative survey (according to the original study design assumptions for the Polish 400 Cities Project).
Statistical analyses were produced using the SAS System for Windows Release 8.02. Simple associations were assessed with frequency tables and Pearson’s chi-squared tests for two independent proportions. Means and medians were calculated to summarize continuous effects and were compared by t-tests.
Results
Age and gender structure
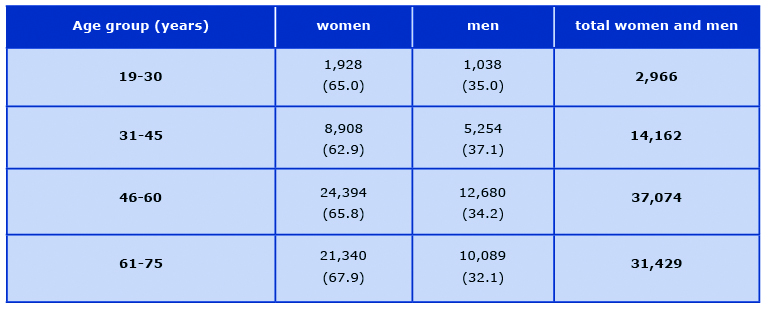
In total, 92385 people reported for the screening tests (61318 female and 31067 male subjects). Of those screened, 7.3% were people older than 75. This means a group of 6,754 people (4748 women and 2006 men) who, according to the study design, were not included in further analyses since they exceeded the upper age limit of the representative survey. The representative survey included in total 1278 subjects (710 women and 568 men). Mean age of subjects in the screening study was 55.3 (SD 12.1), vs. 44.4 (SD 15.7), in the representative survey (p < 0,01). Women accounted for 66.1% of screening study participants, vs. 55.3% in the representative sample. Tables 1 and 2 show the age and gender structure for the representative sample and for the group of screening test participants.
Table 1. Age and gender structure of the sample in the representative survey, number of subjects; (figures in brackets indicate percentages of men and women in each age group)
Table 2. Age and gender structure of volunteers in the screening study, number of subjects; (figures in brackets indicate percentages of men and women in each age group)
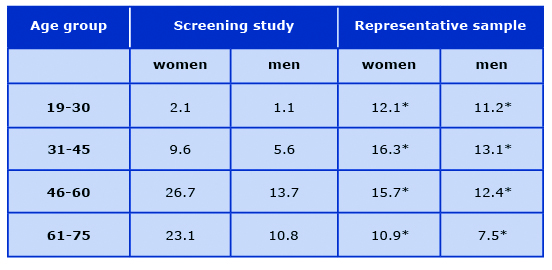
The largest group among the volunteers in the P400CP screening were women aged 46-60 (26.7% of all participants), followed by women aged 61-75 (23.1%). The smallest volunteer group were men aged 19-30 (1.1%). Men aged 31-45 accounted for 5.6% of volunteers. Percentages of the screening study participants in all the groups defined by age and gender differed significantly from those obtained in the representative sample (Table 3).
Table 3. Structure of participants, split by age and gender (in percentages)
*p < 0.05 vs. volunteers in the screening study
Awareness of arterial hypertension, diabetes and hypercholesterolemia
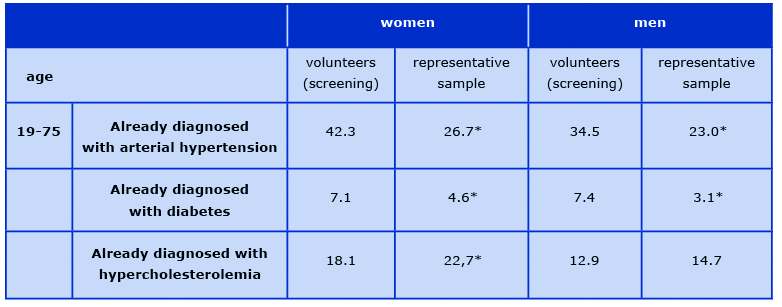
Of the participants in the screening study 39.6% declared previously diagnosed hypertension, vs. 24.8% of respondents in the representative survey (p < 0.001). Over 7% of screening study participants declared previously diagnosed diabetes, compared to ~4% in the representative survey, (p < 0.001). Whereas 16.3% of screening test participants had been already diagnosed with hypercholesterolemia (19% in the representative survey, not statistically significant). Table 4 shows the data split by gender.
Table 4. Awareness of existing (already diagnosed) risk factors in the surveyed groups (data in percentages)
*p < 0.05 vs. volunteers in the screening study
The analysis of the awareness of existing risk factors by age groups (19-30, 31-45, 46-60 and 61-75) did not reveal any statistically significant differences between the population of volunteers in the screening and the control sample. This suggests that higher awareness of existing (already diagnosed) hypertension, diabetes and hypercholesterolemia may be linked to the fact that the age distribution in the group of volunteers was generally skewed towards the older age groups.
Prevalence of newly detected conditions of elevated blood pressure, hyperglycemia and hypercholesterolemia.
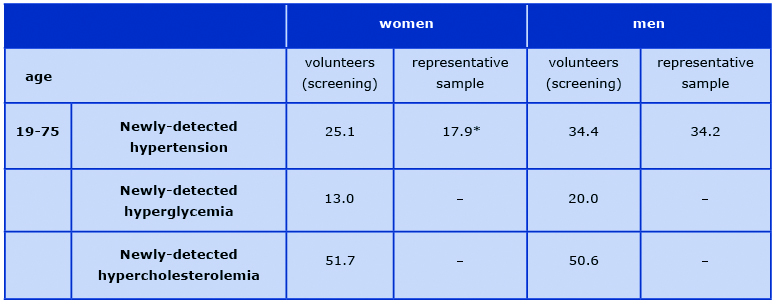
In the screening study elevated blood pressure at the first visit (≥ 140/90 mmHg) was detected in over 28% of the volunteers who did not declare an earlier diagnosis of hypertension. Whereas in the representative sample previously undiagnosed elevated blood pressure was reported in 25.3%. Two-thirds of the volunteers in the screening study who were diagnosed with raised blood pressure for the first time in their life reported for the second visit (control visit) in order to confirm the hypertension diagnosis. Hyperglycemia (≥ 100mg%) was detected in over 15% of screening study participants who had not been earlier diagnosed with diabetes.
Table 5 shows the prevalence of newly-diagnosed carbohydrate metabolism disorders in the group of screening study participants. An increased level of cholesterol (≥ 190 mg/dl) was detected in over 51% of screening study participants unaware of the condition. Data on the prevalence of newly detected risk factors, split by gender, are shown in Table 5.
Table 5. Prevalence of newly detected risk factors in the surveyed groups (data in percentages)
* p < 0.05 vs. volunteers
Prevalence of cigarette smoking
36% of respondents in the representative sample were smokers, compared to 16.5% in the screening study population (p < 0.05). The statistically significant difference exists for men and women alike, and it is also valid across all age groups (Table 6).
Table 6. Prevalence of tobacco smoking in the surveyed groups. (Data shown in percentages)
* p < 0.05 vs. volunteers
Discussion
Many prevention programs targeting cardiovascular diseases were carried out in Poland over a period of the past decade, but their principal component (and quite often the only one) tended to be a screening study. Data collected for the Council of the POLKARD Program reveal that in the years 2004-2005 alone there were 704 screening study programs carried out in Poland, with a total of over 740 thousand participants [15]. The same data indicate that that there are no uniform standards concerning this type of activities. The screening programs differed with regard to the scope of tests, their target groups, or methods used to invite people to participate.
In the P400CP study the screening tests were preceded by a public awareness campaign in the media [16-19]. The campaign provided information about the objective of the study and explained who should participate in the tests (emphasis was placed on those who had not been diagnosed before and on men of working age). On the other hand, it should be emphasized that the screening study had an “open” design. Consequently, any person who received information about the tests and wished to participate was eligible. Due to this recruitment method, men accounted for only one third of participants, and in the group of young males (< 45 years of age) for only 7%; whereas the data obtained from the representative sample indicate that this could have not been caused by the actual demographic structure of the small town population. It seems that in order to redress the gender imbalance in screening programs addressed to both men and women, these programs would need an extensive support of psychology and sociology experts.
The mean age of participants in the screening study was 10 years above the mean age in the control (representative) sample. This might, to a certain extent, result from the fact that the test hours for taking blood pressure, fasting glycemia and cholesterolemia readings were scheduled for mornings (for obvious reasons), This schedule could have been inconvenient for those participants who were employed, despite the fact that screening points in many towns were open on a Saturday as well. When planning and organizing future screening programs, this issue must be taken into account.
An analysis of hypertension-related data indicates that as much as 40% of screening test participants declared a condition which had been diagnosed before. Including these subjects in screening tests is somewhat contradictory to the core concept of screening, even though their participation allows drawing conclusions about hypertension control in the population. After all, collecting hypertension control data should not be the objective of screening tests. On the other hand, the results of the control survey indicated that as much as a quarter of the representative small-town population were unaware of their hypertensive condition, which gives a well-founded rationale for widely designed screening in the target population. In the screening study the proportion of subjects diagnosed with elevated blood pressure for the first time in their lives reached almost 30% of participants. These people were invited for a second visit, to confirm the diagnosis [20-21]. However, only two thirds of this group took the opportunity of a second visit. This is an indicator of the need to develop tools that would effectively motivate patients to complete the full diagnostic process. When carbohydrate metabolism disorders are analyzed, conclusions similar to those valid for arterial hypertension may be drawn.
The age difference between the screening study population and the representative sample resulted in a much higher awareness of existing hypertension or diabetes in the former group. This does not apply to hypercholesterolemia, for which no statistically significant differences were detected between the groups. If we analyze the female population only, the awareness of hypercholesterolemia was more often declared in the representative sample. This seems to be a result of a generally very low awareness of hypercholesterolemia, despite the fact that this condition is the risk factor with the highest prevalence [5]. While only 16% of participants in the screening study declared previously diagnosed hypercholesterolemia, the condition was diagnosed for the first time in over half of the screened group. This, in turn, indicates that an “open” design of the screening study provides the most effective format when screening for hypercholesterolemia in the small-town population.
Interesting results were obtained with regard to the prevalence of cigarette smoking. In the representative survey the proportion of male smokers in small towns exceeds 47%, whereas in the screening study smoking was much less prevalent, among both men and women and across all age groups. We may hypothesize that non-smoking and taking part in screening tests are both an expression of a health-conscious attitude, and this the reason why non smokers are overrepresented in the screening. Therefore, anti-nicotine activities in small towns should be primarily based on measures extending beyond screening, such as social campaigns and education.
To conclude, it should be emphasized that, despite their limitations, screening programs are effective in improving the detection of risk factors. In the group of over 90 thousand participating volunteers, the screening study revealed many previously undiagnosed cases of raised blood pressure, carbohydrate metabolism disorders and, specifically, hypercholesterolemia. On the other hand, the “open” design of screening does not fully accomplish the assumed objective of reaching the hard-to-include group, i.e men under 45. This should be taken into consideration when planning future cardiovascular prevention programs.
Conclusions
“Open” screening programs do not ensure adequate access to the sub-population of young adults, especially males aged up to 45, despite social campaigns addressed specifically to this group, whereas those who willingly participate in “open” screening tests are older people, often already diagnosed with arterial hypertension and diabetes. However, regardless of these limitations, “open” screening tests are a useful tool, as they help to identify many newly detected cases of hypercholesterolemia – a widespread condition of which awareness is low. A similar situation, even though to a lesser extent, occurs also in the case of hypertension. People reporting for screening tests are more often non-smokers, whereas prevalence of smoking in the control population is much higher, especially among men. This, in turn, points out that there is a specific need to develop methods of effective anti-tobacco intervention in small towns in Poland.
Acknowledgements
P400 CP working group: Bogdan Wyrzykowski, Tomasz Grodzicki, Andrzej Januszewicz, Krzysztof Narkiewicz, Marzena Zarzeczna-Baran, Jerzy Głuszek, Grzegorz Opolski, Witold Zatoński, Andrzej Tykarski, Wojciech Drygas.
The Polish 400 Cities Project was financed by the Polish Ministry of Health as a part of the National Cardiovascular Disease Prevention and Treatment Program POLKARD 2003-2008 and by unrestricted educational grants from (in random order): Polpharma, Servier, Sanofi Aventis, GZF Polfa, Pfizer.
References
| 1. |
Podstawowe informacje o rozwoju demograficznym Polski w latach 2000-2009 [Internet]. Główny Urza̦d Statystyczny Departament Badań Demograficznych; [cited 2021 Feb 5]. Available from: http://stat.gov.pl/cps/rde/xbcr/gus/lu_podsta_info_o_rozwoju_demograf_polski_2000-2009.pdf.
|
| 2. |
Rocznik demograficzny. Warszawa: Główny Urza̦d Statystyczny; 2006.
|
| 3. |
Wojtyniak B, Goryński P, Seroka W. Stan zdrowia ludności Polski na podstawie danych o umieralności. In: Sytuacja Zdrowotna Ludności Polski. Warszawa: Państwowy Zakład Higieny – Zakład Statystyki Medycznej; 2003. p. 21–9.
|
| 4. |
Wojtyniak B, Goryński P, Rabczanko D, et al. Umieralność przedwczesna i ogólna z powodu chorób układu krążenia w Polsce na tle sytuacji w Unii Europejskiej, Europie i USA. Warszawa: Państwowy Zakład Higieny; 2007.
|
| 5. |
Zdrojewski T, Bandosz P, Szpakowski P i wsp. Rozpowszechnienie głównych czynników ryzyka chorób układu sercowo-naczyniowego w Polsce. Wyniki badania NATPOL PLUS. Kardiol Pol. 2004;61(supl 4):1–26.
|
| 6. |
Rada Programu POLKARD 2003-2005. Narodowy Program Profilaktyki i Leczenia Chorób Układu Sercowo-Naczyniowego POLKARD 2003-2005. Warszawa; 2003.
|
| 7. |
Podolec P, Karch I, Pająk A, Kopeć G, Broda G, Drygas W, et al. Najważniejsze polskie programy epidemiologiczne i prewencyjne. In: W: Podolec P(red) Podręcznik Polskiego Forum Profilaktyki. Kraków; 2007. p. 103–10.
|
| 8. |
Programy profilaktyczne / Dla Pacjenta / Narodowy Fundusz Zdrowia (NFZ) – finansujemy zdrowie Polaków [Internet]. [cited 2021 Feb 5]. Available from: https://www.nfz.gov.pl/dla-pacjenta/programy-profilaktyczne/.
|
| 9. |
Zdrojewski T, Rutkowski M, Zarzeczna-Baran M, Grodzicki T, Januszewicz A, Narkiewicz K, et al. Ogólnopolski, wieloośrodkowy program profilaktyki chorób układu krążenia: Polski Projekt 400 Miast: główne założenia, cele oraz sposób realizacji. Pol Przegląd Kardiol. 2004;6(4):423–30.
|
| 10. |
Zdrojewski T, Ignaszewska-Wyrzykowska A, Wierucki Ł, Januszko W, Szpajer M, Krupa-Wojciechowska B. Modelowy projekt prewencji chorób układu krążenia na przykładzie doświadczeń Programu SOPKARD. Część pierwsza. Chor Serca i Naczyń [Internet]. 2004;1(2):115–29. Available from: https://journals.viamedica.pl/choroby_serca_i_naczyn/article/view/12231.
|
| 11. |
Wilson JMG, Jungner G, Organization WH. Principles and practice of screening for disease. Public Heal Pap Number [Internet]. 1968;(34). Available from: https://apps.who.int/iris/bitstream/handle/10665/37650/WHO_PHP_34.pdf.
|
| 12. |
Windak A, Godycki-Ćwirko M, Windak A. Wytyczne Polskiego Forum Profilaktyki dotyczące badań przesiewowych w profilaktyce chorób układu krążenia. In: Podolec P, editor. Podręcznik Polskiego Forum Profilaktyki. Medycyna Praktyczna; 2007. p. 721–2.
|
| 13. |
Perk J, De Backer G, Gohlke H, Graham I, Reiner Z, Verschuren M, et al. European Guidelines on cardiovascular disease prevention in clinical practice (version 2012): The Fifth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by re. Eur Heart J [Internet]. 2012 Jul 1;33(13):1635–701. Available from: https://academic.oup.com/eurheartj/article-lookup/doi/10.1093/eurheartj/ehs092.
|
| 14. |
Zdrojewski T, Wyrzykowski B, Wierucki L, Grodzicki T, Januszewicz A, Narkiewicz K, et al. Attempt to eliminate health inequalities in Poland arising at the time of political and economic transformation: Polish 400 Cities Project. Eur J Cardiovasc Prev Rehabil [Internet]. 2006 Oct 28;13(5):832–8. Available from: https://doi.org/10.1097/01.hjr.0000239472.33756.e6.
|
| 15. |
Hanke W, Drygas W, Pasowicz M, et al. Opracowanie modelu organizacyjnego i prawnego badań przesiewowych w zakresie czynników ryzyka chorób układu krążenia, uwzględniającego aktualne standardy medyczne i sytuację społeczno-ekonomiczną w Polsce. Projekt przygotowany na zamówienie Rady Programu. Warszawa; 2003.
|
| 16. |
Bellicha T, McGrath J. Mass media approaches to reducing cardiovascular disease risk. Public Health Rep [Internet]. 1990;105(3):245–52. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1579998/.
|
| 17. |
Beaudoin CE, Fernandez C, Wall JL, Farley TA. Promoting Healthy Eating and Physical Activity. Am J Prev Med [Internet]. 2007 Mar;32(3):217–23. Available from: https://doi.org/10.1016/j.amepre.2006.11.002.
|
| 18. |
Snyder LB. Health Communication Campaigns and Their Impact on Behavior. J Nutr Educ Behav [Internet]. 2007 Mar;39(2):S32–40. Available from: https://doi.org/10.1016/j.jneb.2006.09.004.
|
| 19. |
Drygas W, Słońska Z, Torbicki A, et al. Kampanie medialne w promocji zdrowia i profilaktyce chorób serca i naczyń – doświadczenia międzynarodowe. In: Podręcznik Polskiego Forum Profilaktyki. 2007. p. 131–4.
|
| 20. |
Chobanian A V, Bakris GL, Black HR, Cushman WC, Green LA, Izzo Joseph L. J, et al. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood PressureThe JNC 7 Report. JAMA [Internet]. 2003 May 21;289(19):2560–71. Available from: https://doi.org/10.1001/jama.289.19.2560.
|
| 21. |
Committee G. 2003 European Society of Hypertension–European Society of Cardiology guidelines for the management of arterial hypertension. J Hypertens [Internet]. 2003;21(6):1011–53. Available from: https://journals.lww.com/jhypertension/Fulltext/2003/06000/New_year,_new_challenges.1.aspx.
|
