

Commentary on: The usefulness and limitations of diffusion tensor imaging – a review study


Citation
Szmuda T, Ali S. Commentary on: The usefulness and limitations of diffusion tensor imaging – a review study. Eur J Transl Clin Med. 2019;2(2):85-86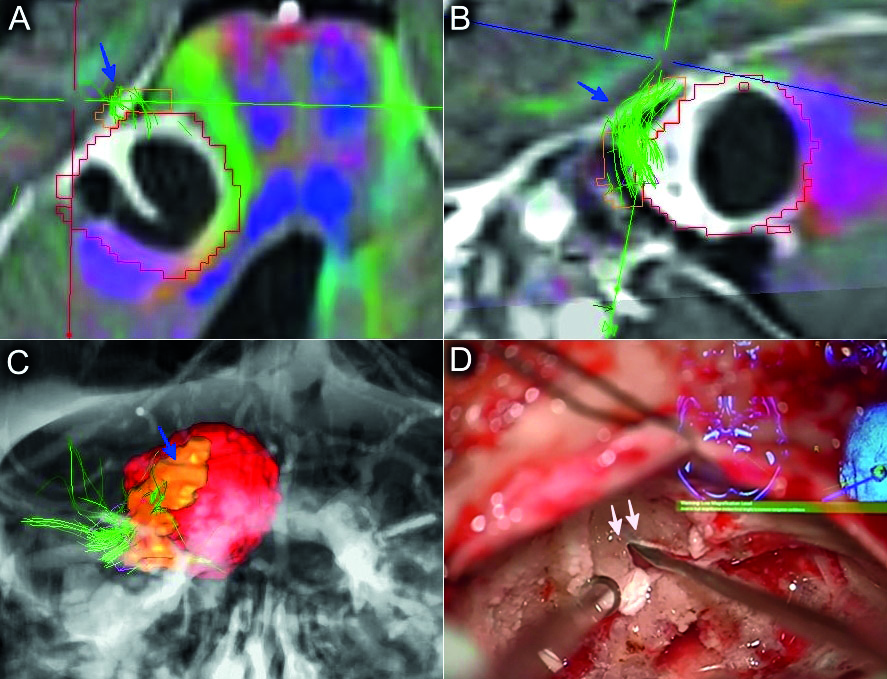

Abbreviations and acronyms
CPA – cerebello-pontine angle
DTI – diffusion tensor tractography
FN – Facial nerve
Dear Editor,
We read with great enthusiasm the review article by Sara Kierońska and Paweł Słoniewski about the limitations of diffusion tensor imaging (DTI) [1]. While it was brilliant, we felt that the paper could have benefitted from alluding to the role DTI of cranial nerves in cerebello-pontine angle (CPA) tumours.
If the facial nerve (FN) surrounds a tumour, it should be always preserved during a large CPA tumour surgery, although, sometimes it cannot be visualised intraoperatively. In such cases DTI might be particularly helpful. As researchers at the Medical University of Gdańsk, we were among the first to attempt FN tracking with DTI, however we obtained suboptimal results [2]. A 2018 systematic review on 234 cases, reported only a 90.6% accuracy of FN identification by fibre tracking DTI. For reference, the prediction rate of the FN’s position in CPA tumours should reach 100% [3]. The current imaging capabilities of DTI are unsatisfactory and neurosurgeons should strive for better outcomes especially since concurrent radiosurgery enables similar CPA tumour control. At our department we tracked the FN in the operating room by integrating preoperative planning with a real-time neuronavigation system. This initially promising hypothesis, still unpublished, was ultimately disappointing as the prediction rate of about 80% was lower than expected.
Figure 1. Facial nerve’s path tracked by diffusion tensor imaging as it courses around the vestibular schwannoma.
A – axial planes, B – sagittal planes (green bundles), C – a three-dimensional model (segmented in orange volume), D – the debulking of the acoustic canal
Figure 1: The image illustrates the facial nerve’s path tracked by diffusion tensor imaging as it courses around the vestibular schwannoma. Facial nerve predictions are presented on axial (A) and sagittal planes (B) (green bundles) and on a three-dimensional model (C) (segmented in orange volume). The debulking of the acoustic canal is presented in the intraoperative snapshot (D), the picture is injected to the screen is shown in the right upper corner.
In cases where the accuracy of DTI is moderate, a combination of DTI with other imaging modalities might yield more reliable results. For instance, Pereira et al. complemented standard DTI with multiplanar fused sequences of magnetic resonance imaging; they took advantage of the regularity that only tumours enhanced with contrast could offer and thereby they isolated the surrounding cranial nerves [4]. This study of six patients postulates that the combined imaging with standard DTI could improve operative planning. While still a preliminary study, the agreement between the fused imaging and actual intraoperative anatomy proved to be correct always. We encourage scientists to experiment by combining the imaging potential of multiple modalities like DTI and magnetic resonance imaging. Perhaps together they can yield more accurate results than if used alone.
Regardless of our assessment, the study by Kierońska et al. contributes a relevant and critical appraisal of DTI. Radiological imaging like DTI is central to neurological surgery and we commend the authors for reviewing the limitations of it. We hope our commentary expands the scientific discourse on this topic, thus serving as another building block to advance the imaging standards of neurosurgery.
References
| 1. |
Kierońska S, Słoniewski P. The usefulness and limitations of diffusion tensor imaging – a review study. Eur J Transl Clin Med [Internet]. 2019 Oct;2:[ahead of pub]. Available from: https://doi.org/10.31373/EJTCM/112437.
|
| 2. |
Szmuda T, Słoniewski P, Sabisz A, Szmuda M. Traktografia nerwu twarzowego w guzach kąta mostowo-móżdżkowego. Otorynolaryngologia [Internet]. 2014;13(1):42–50. Available from: https://www.otorynolaryngologia-pk.pl/f/file/orl-2014_vol-13_issue-1_article-1136.pdf.
|
| 3. |
Savardekar AR, Patra DP, Thakur JD, Narayan V, Mohammed N, Bollam P, et al. Preoperative diffusion tensor imaging–fiber tracking for facial nerve identification in vestibular schwannoma: a systematic review on its evolution and current status with a pooled data analysis of surgical concordance rates. Neurosurg Focus [Internet]. 2018 Mar;44(3):E5. Available from: https://doi.org/10.3171/2017.12.FOCUS17672.
|
| 4. |
Pereira PG, Manacas R. Magnetic Resonance Imaging Fusion of Cranial Nerves Impaired by Skull Base Tumors: A Technical Development. J Nucl Med Radiat Ther [Internet]. 2019;10(1):396. Available from: https://doi.org/10.4172/2155-9619.1000396.
|
